




Abstract
Aims
Perthes’ disease is a condition leading to necrosis of the femoral head. It is most common in children aged four to nine years, affecting around one per 1,200 children in the UK. Management typically includes non-surgical treatment options, such as physiotherapy with/without surgical intervention. However, there is significant variation in care with no consensus on the most effective treatment option.
Methods
This systematic review aims to evaluate the effectiveness of non-surgical interventions for the treatment of Perthes’ disease. Comparative studies (experimental or observational) of any non-surgical intervention compared directly with any alternative intervention (surgical, non-surgical or no intervention) were identified from: Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMcare, Allied and Complementary Medicine Database (AMED), and the Physiotherapy Evidence Database (PEDro). Data were extracted on interventions compared and methodological quality. For post-intervention primary outcome of radiological scores (Stulberg and/or Mose), event rates for poor scores were calculated with significance values. Secondary outcomes included functional measures, such as range of movement, and patient-reported outcomes such as health-related quality of life.
Results
In all, 15 studies (1,745 participants) were eligible for inclusion: eight prospective cohort studies, seven retrospective cohort studies, and no randomized controlled trials were identified. Non-surgical interventions largely focused on orthotic management (14/15 studies) and physical interventions such as muscle strengthening or stretching (5/15 studies). Most studies were of high/unknown risk of bias, and the range of patient outcomes was very limited, as was reporting of treatment protocols. Similar proportions of children achieving poor radiological outcomes were found for orthotic management and physical interventions, such as physiotherapy or weightbearing alteration, compared with surgical interventions or no intervention.
Conclusion
Evidence from non-randomized studies found no robust evidence regarding the most effective non-surgical interventions for the treatment of children with Perthes’ disease. Future research, employing randomized trial designs, and reporting a wider range of patient outcomes is urgently needed to inform clinical practice.
Cite this article: Bone Jt Open 2020;1-12:720–730.
Take home message
Evidence from non-randomized studies found no robust evidence regarding the most effective non-surgical interventions for the treatment of children with Perthes’ disease.
Future research, employing randomized trial designs, and reporting a wider range of patient outcomes, is urgently needed to inform clinical practice.
Introduction
Perthes’ disease is a condition of unknown aetiology that causes hip pain and disability in children.1 It is most common in those aged four to nine years, and boys are four-times more likely to be affected than girls.2 Overall, this disease affects around one per 1,200 children in the UK, but children from parents of low socioeconomic status may be disproportionately affected.3
The first stage of the disease is characterized by a temporary disruption in blood supply causing the femoral head to become necrotic.4 Over time, the damaged bone is reabsorbed and new bone is generated.5 The femoral head eventually heals, but during the disease process, deformity can develop, typically leading to gait disturbance, restricted mobility, pain, and reduced physical activity.6 Occasionally the hip deformity is so severe that the child may require a total hip arthroplasty,7 although surgery is generally only considered once skeletal maturity has been reached in late adolescence.8
Treatments for Perthes’ disease aim to maintain the optimum local environment in and around the hip joint for self-healing to occur with minimal deformity of the femoral head.9,10 Traditionally, non-surgical treatment options include orthotic management (e.g. braces and callipers), physical interventions such as strengthening and stretching regimes, walking aids, activity modification, or watchful waiting.11,12 In recent decades, surgery has also often been considered.7 In the absence of clinical guidelines, there is currently no standardized approach to treatment selection.
Given the life-long impact of Perthes’ disease, the British Society for Children’s Orthopaedic Surgery (BSCOS) consensus exercise, and a separate James Lind Alliance Priority Setting Partnership, have identified Perthes’ disease management as one of the highest priorities for research.13-15
The aim of this review was to evaluate the use of any non-surgical treatment for Perthes’ disease, seeking comparisons to other surgical or non-surgical interventions.
Methods
A protocol for this systematic review was registered with the international prospective register of systematic reviews (PROSPERO).16
Search strategy
The following electronic databases were searched from inception: Cochrane Central Register of Controlled Trials (The Cochrane Library 2019, Issue 7, July 2019); MEDLINE (1946 to July 2019) using ProQuest via the NICE HDAS interface; EMBASE (1974 to July 2019) using ‘disease’ and ‘physical therapy’. Reference lists of potentially eligible studies were reviewed, and citation tracking was used to identify additional studies.
Study selection criteria
Studies designed to compare the effects of a non-surgical intervention with a comparator group were eligible for inclusion. This could include experimental designs - i.e. controlled clinical trials (randomized, quasi-randomized, or non-randomized allocation) or longitudinal observational studies (cohort studies). Systematic reviews, cross-sectional studies with reporting restricted to post-surgical outcomes, case-control studies, and ‘before and after’ observational studies were excluded.
Eligible studies recruited children aged 16 years and under with a radiologically-confirmed diagnosis of Perthes’ disease. Participants were treated with a non-surgical intervention, including physical interventions such as physiotherapy or weightbearing modification, or management with an orthotic device. Studies were excluded if an English full-text version was not available.
Screening
One author (AG) screened all titles and selected an initial ‘long list’ of potentially eligible studies. These abstracts were independently reviewed by two authors (AG, TVH) to confirm potential eligibility, with any discrepancies adjudicated by a third reviewer (CC). Full-text articles were obtained for all short-listed studies and reviewed for eligibility by two authors (AG, TVH).
Data extraction
A standardized data extraction proforma was used to extract data (AG) from eligible studies, including year of publication, country of origin, study design, duration of follow-up period, and sample size available for analysis. Participant details that were extracted include the number of children recruited and completing each follow-up, number of hips (to account for cases of bilateral Perthes’ disease), and age (range) at onset or diagnosis of Perthes’ disease.
Radiological, functional, and patient-reported outcomes were extracted when reported. The primary outcome was the post-intervention radiological shape of the hip when the participant had reached skeletal maturity. Radiological shape was categorized using the Stulberg6 and/or Mose17 classification methods for Perthes’ disease that are commonly used in practice. Event rate data were extracted, with an event defined as a Stulberg rating of ‘4 or 5’ (indicating a poor outcome) and/or categorized by the authors as ‘poor’ using the Mose method of classification, foor which outcomes are ‘poor’ when there is a variation of more than 2 mm when assessing the sphericity of the femoral head.17 To standardize data for comparison across studies, event rates were calculated as the proportion of children with a poor outcome, over the total number of children in the intervention group. Using the frequency data extracted from the papers, two-way tests for differences in proportions for independent groups were calculated (α = 0.05) using the immediate commands in Stata v15 (StataCorp, College Station, Texas, USA).
Secondary outcome data included objective measures of function, such as goniometer measures of range of movement (ROM) at the hip joint, lower limb muscle strength measured on the Oxford scale,18 and gait quality scores (e.g. the “12-minute walk” or the presence of a Trendelenburg sign). For these functional measures, the differences between the two limbs (affected and unaffected) were analyzed. We also extracted any available patient-reported health related quality of life outcomes.
Methodological quality assessment
Although randomized controlled trials were eligible for inclusion, no such studies were identified, so the Cochrane Risk of Bias criteria tool was not used.19 Instead, the Newcastle Ottawa Scale (NOS), designed to assess quality and risk of bias in non-randomized studies,20,21 was applied. The NOS uses a points system to judge three domains: selection, comparability, and outcome, with a maximum score of eight points. A risk of bias score is then allocated according to the overall number of points, categorized as ‘high’ (0 to 3 points), ‘moderate’ (4 or 5 points), or ‘low’ (6 to 8 points).22 One author (AG) scored each study, while a second author (TVH) independently verified the scoring.
To assess the quality of reporting of the study interventions, the Template for Intervention Description and Replication (TIDieR) checklist was used, with data extracted by one author (AG). This 12-point scale has a maximum of two points available for each category, with an overall potential score of 24. Higher scores indicate that the quality of reporting is more likely to aid implementation or replication of the interventions.20 The TIDieR tool is becoming a widely recognized measure of the completeness of intervention reporting within studies.23,24
Analysis
A narrative synthesis was undertaken because studies were deemed too clinically and/or methodological heterogeneous for statistical pooling of data. The first stage of analysis was to develop a typology of the non-surgical interventions evaluated, with each intervention classified as either a physical intervention or orthotic management. The results were then stratified by the type of interventions being compared. For example, we grouped studies comparing orthotic management with another non-surgical intervention separately from studies comparing orthotic management to a surgical intervention comparator. Data with similar outcomes were then synthesized within each of these groups.
Results
Study selection
Electronic database searches identified 8,795 records (including duplicates). A PRISMA diagram of the review process is provided in Figure 1.25 After screening titles and abstracts, 32 full-texts were considered, and ultimately 15 studies were included in the review (Table I). Orthotic management includes any orthoses, calliper, or casting used. Comparators could include another non-surgical intervention or a surgical intervention (i.e. femoral or pelvic osteotomies, or surgery to the soft tissue or muscular/tendons). Physical interventions include treatments such as stretching, both active and passive, strengthening, and also treatments such as weightbearing modification.
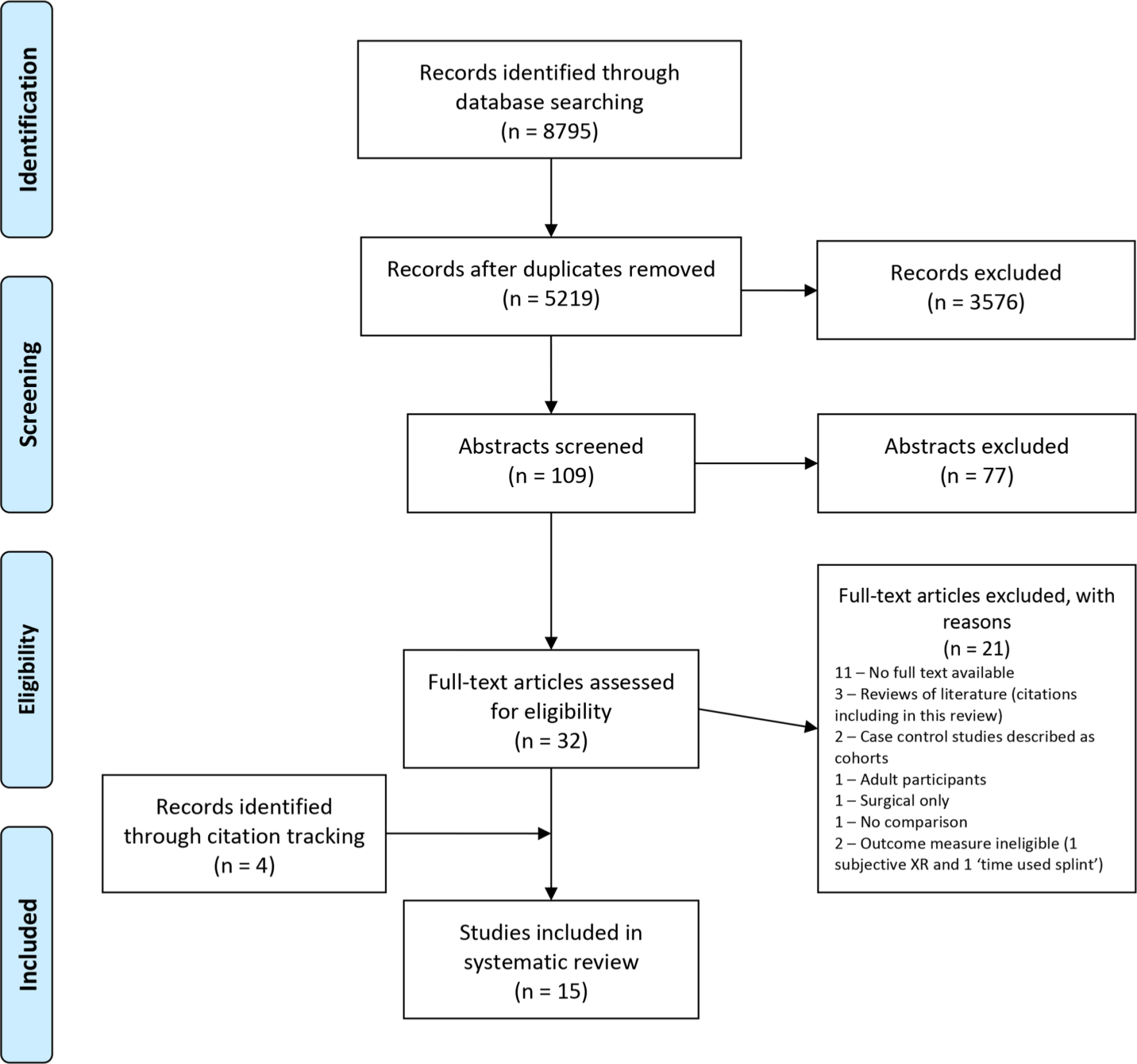
Fig. 1
PRISMA flow chart showing literature search process.
Table I.
Summary of studies included in review.
| Author(s) | Study design (length of follow-up) |
Setting | Children, hips (n) | Age at onset (range) |
Intervention(s)and treating clinician* | Comparator | Primary outcome(s) | Secondary outcomes | NOS score | TIDieR score |
|---|---|---|---|---|---|---|---|---|---|---|
| Askoy 2004 Turkey26 |
Retrospective cohort (10 to 33 years) |
Not reported | 48 (51) Int: 23 (23) Comp: 25 (28) |
6 to 9 years | Braced† (mean time 14 months; range 12 to 18 months) | Non-braced | Stulberg | N/A | 4 | 11 |
| Arkader 2008 Brazil27 |
Retrospective cohort (5 to 22 years) |
Not reported | 43 (43]) Int: 22 (22) Comp: 22 (22) |
9 to 14 years | Multi-component (Orthotic (brace) with physiotherapy if needed) Treating clinician - physical therapist for input. |
Surgical (FVO or Chiari osteotomy) | Stulberg | N/A | 4 | 6 |
| Brech 2006 Brazil28 |
Prospective cohort (12 weeks) |
Physiotherapy clinic | 17 (17) Int: 8 (8) Comp: 9 (9) |
3 to 8 years | Physiotherapy (Stretches, strengthening and balance - 12 weeks) Treating clinician - Physiotherapist |
Active observation | N/A | ROM | 7 | 13 |
| Citlak 2012 Turkey29 |
Retrospective cohort (8 to 25 years) |
Not reported | 25 (27) Int: 14 (16) Comp: 11 (11) |
6 to 8 years | Orthotic (Thomas splint) (mean time 16.3 months; range 4 to 24 months). |
Surgical (FO) | Stulberg | IOWA Scale questionnaire |
4 | 8 |
| Cooperman 1984 Sweden, USA, Yugoslavia, Israel30 |
Multicentre retrospective cohort (3 to 25 years) |
Not reported (hospital names provided) |
248 (248) Int1: 48 (48) Int2: 58 (58) Int3: 72 (72) Comp: 70 (70) |
2 to 15 years | Int1: Orthotic (NAO) Int2: Orthotic (SRO) Int3: Crutches (no data on treatment time) |
Surgical (FO) | Subjective radiograph review | N/A | 4 | 9 |
| Edvarson 1981 Norway31 |
Prospective cohort (3 to 13 years) |
Not reported (hospital) |
58 (63) Int: 28 (32) Comp: 30 (31) |
2 to 11 years | Bed rest/sling (Bed rest mean 9 months, sling mean 18 months, no ranges reported) |
Surgical (VO) | Mose | Gait assessment (Trendel-enburg) | 3 | 13 |
| Evans 1988 USA32 |
Retrospective cohort (4 to 10 years) |
Not reported (hospital) |
36 (36] Int: 17 (17) Comp: 19 (19) |
5 to 12 years | Orthotic (NAO) (range 8 to 42 months) |
Surgical (VDO) | Mose | ROM | 4 | 11 |
| Fulford 1993 Scotland33 |
Prospective cohort (3 to 6 years) |
Paediatric surgical unit | 94 (99) Int: 42 (43) Comp: 52 (56) |
4 to 10 years | Traction (6 weeks) followed by orthotic (abduction calliper) (Mean 20 months, range 8 to 32 months) |
Traction followed by surgery (osteotomy and plate insertion) | No Stulberg or Most (used Caterall) | 12 min walk | 4 | 14 |
| Herring 2004 USA34 |
Multicentre prospective cohort (1 to 15 years) |
Not reported | 337 (345) Int1: (129) Int2: (27) Int3: (19) Comp: 120 (no. of children not given for each intervention group) |
6 to 12 years | Int1: Orthotic (SRO) (no timeframes reported but instruction to wear until radiological re-ossification) Int2: ROM exercises (standing abduction stretch and active ROM once a day, no duration of regime reported) Int3: No treatment (symptom relief only) |
Surgery (FO or IO; 52 and 68 respectively) | Stulberg | Modified Pillar Classi-fication | 7 | 12 |
| Jani 1980 Switzerland35 |
Prospective cohort (follow-up data missing)‡ |
Not reported | 83 (83) Int1: 19 (19) Int2: 40 (40) Comp: 24 (24) |
Age not reported | Int1: Traction and orthosis (orthosis not described, or regime reported) Treating clinician – not specified Int2: Conservative (Int1) with surgery if symptoms develop. |
Surgery (VO) with Physiotherapy post-op (regime not reported) | No Stulberg or most (used Caterall) | N/A | 7 | 6 |
| Marklund 1976 Sweden36 |
Prospective cohort (follow-up data missing)§ |
Not reported (hospital) |
47 (49) Int: 22 (23) Comp: 25 (26) |
2 to 11 years | Conservative management; bed rest ± traction and Thomas splint until radiological re-ossification was observed (range 1 to 3 years) | Surgical (sub-trochanteric osteotomy) | Subjective radiograph review | N/A | 4 | 7 |
| Osman 2009 Scotland37 |
Retrospective cohort (2 to 20 years) |
Not reported (hospital) | 44 (48) Int1: 12 Int2: 14 Comp: 22 (no. of children not given for each intervention group) |
8 to 14 years | Int1: Orthotic (abduction cast) Int2: No treatment (no regimes reported) |
Surgical (FVO or Shelf osteotomy; 4 and 18 respectively) | Stulberg Mose |
N/A | 5 | 9 |
| Poussa 1993 Finland38 |
Retrospective cohort (2 to 16 years) |
Not reported (hospital) |
218 (232) Int: 96 (116) Comp: 112 (126) |
5 to 13 years | Conservative; orthosis (Thomas splint) or crutches (no time frame specified) | Surgical (FO) | Subjective radiograph review | N/A | 6 | 6 |
| Wang 1995 USA39 |
Prospective cohort (2 to 27 years) |
Not reported | 124 (141) Int1: 38 (41) Int2: 38 (41) Int3: 23 (29) Comp: 25 (30) |
2 to 12 years | Int1: Orthotic (SRO) (Mean time 8 months, range 1 to 20 months) Int2: NWB and exercises (Included bedrest, crutches, or callipers to prevent weightbearing on the affected hip, no regime reported) Int3: Orthotic (Petrie cast) (no regime reported) |
Surgical (FVO or Salter osteotomy; 15 each) | Stulberg Mose |
N/A | 8 | 10 |
| Wiig 2008 Norway40 |
Multicentre prospective cohort (5 years) |
Not reported | 323 (323) Int1: 27 (27) Int2: 220 (220) Comp: 76 (76) |
1 to 15 years | Int1: Orthotic (SRO) (No timeframes given) Int2: Physiotherapy (range of movement exercises with special emphasis on abduction, internal rotation and extension, in addition to muscle strengthening exercises) |
Surgical (FVO) | Modified 2-group Stulberg | N/A | 7 | 10 |
-
*
Treating clinician not specified unless listed.
-
†
Brace not specified other than ‘trilateral socket hip abduction orthosis’.
-
‡
rReported “until disease process complete”.
-
§
Reported as “primary end result”.
-
¶
Reported that “all were mature at follow-up”.
-
AHI, acetabular head index; ATD, articulotrochanteric distance; Comp, comparison; FO, femoral osteotomy; Int, intervention; IO, innominate osteotomy; NAO, Newington abduction orthosis; NOS, Newcastle Ottawa Scale; ROM, range of movement; SAR, slope of acetabular roof; SRO, Scottish Rite orthosis; TIDieR, template for intervention description and replication; VDO, varus derotational osteotomy; VO, varus osteotomy.
Quality assessment
NOS risk of bias scores ranged from 3 to 8 out of 8 (Table I) with 1/15 assessed as high risk, 8/15 assessed as moderate risk, and 6/15 as low risk. The most common quality issues identified were inadequate description of follow-up and failure to consider or control for potential confounders. Interventions were generally poorly described, with TIDieR scores ranging from 6 to 14 out of 24 (Table I). Study scores were reduced because they failed to report intervention procedures including materials, dosage and who carried out the intervention. A more detailed description of how the NOS and TIDieR scores are categorized is presented in supplementary Tables 1 and 2.
Characteristics of included studies
All 15 included studies recruited children with a radiological diagnosis of Perthes’ disease, providing a total of 1745 participants (Table I).26-40 Sample sizes ranged from 17 children28 to 337 children,38 and the age of children at onset of symptoms ranged from one to 15 years old. One study followed children up for 12 weeks.28 Otherwise, children were followed up for a minimum of one year33 and a maximum of 33 years.26
In terms of study design, there were two multicentre prospective cohort studies,34,40 six single-centre prospective cohort studies,28,31,33,35,36,39 one multicentre retrospective cohort study30 and six retrospective cohort studies.26,27,29,32,37,38
Interventions compared
A range of non-surgical interventions were evaluated within the 15 studies and 13 included a surgical comparison group.27,29-40 With regards to non-surgical interventions, four studies included an intervention group that consisted of ‘active observation.’26,28,34,37
Orthotic management (including callipers, braces, casts and any other orthoses) was evaluated in 14/15 studies.26,27,29-40 Physical interventions (including strengthening exercises, stretching exercises, and/or mobility adaptation such as altered weightbearing statuses and balance work) were reported in 5/15 studies.28,30,38-40 One study reported that a group was managed ‘conservatively with theatre if at risk’, but the conservative management protocol was not described.35
Four studies included at least one comparator intervention comprising multiple treatment components.26,27,33,36 Two of these studies combined either a brace26 or a cast after surgical intervention (tenotomy)27 with physiotherapy if clinically indicated. A third study compared two groups with traction and either calliper application or surgery.33 A fourth included two multicomponent groups: traction and orthosis; and surgery followed by physiotherapy.36
Primary outcomes
Six studies applied the Stulberg classification26,27,29,34,39 and four studies used the Mose classification,31,32,36,37 with two studies measuring both these radiological outcomes.36,37 Two of the studies reported a ‘modified’ Stulberg score which combined Stulberg categories 1 and 2 to create a new category for a favourable outcome, and combined Stulberg categories 4 and 5 to create a new category for a poor outcome. Category 3 remained unchanged, equating to a ‘fair/moderate’ outcome.26,38 Five other studies reported relevant interventions but without using objective radiological outcome measures that could be synthesized (data not reported).28,33,35,36,38 Two papers did not report the primary outcomes; however, given the relevance of the study to this review they were included.36,38
Secondary outcomes
Functional outcomes were reported in four studies: two reported ROM outcomes,28,32 one described a muscle strength outcome (Oxford scale),28 and one study had used the 12-minute walk test to assess gait quality in children pre- and post-intervention.33 Only one study reported patient health-related quality of life, but the authors did not state what questionnaire was used or previously validated in this population.29 The authors also failed to give details on when it was used, stating ‘at clinical assessment each patient answered a questionnaire’, and they provided no more information as to how frequently these clinical assessments took place.
Studies comparing orthotic management with no intervention or surgery
The primary outcomes (Stulberg and/or Mose score) for studies comparing orthotic management with the comparator of no intervention (three studies26,34,37) or surgical repair (nine studies27,29,30,32,34,37-40) are presented in Tables II and III. Although the treatment protocol in all of these studies mandated orthotic management, two studies also provided supplementary physiotherapy input ‘if needed’; 47%26 and 40%27 of children received supplementary physiotherapy input respectively. Comparing orthotic management with no intervention, all studies reported similar proportions of children with poor radiological outcomes between groups.26,34,37 When orthotic management was compared with surgical intervention, findings across the nine studies included in our review were inconsistent. One study that compared surgery with two different types of orthosis treatments39 reported a greater proportion of children with favourable outcomes for children managed with a Petrie cast orthosis compared to those undergoing surgery (p < 0.05), but no difference between surgery and Scottish Rite orthosis management. In contrast, a later study40 reported a greater proportion of children with poor radiological outcomes after orthotic management compared to surgical treatment (p < 0.05). The remaining six studies27,29,31,32,34,37 found no between group differences.
Table II.
Physical and orthotic interventions: Primary outcome assessed using Stulberg method.
| Author | Children, hips (n) | Intervention | Intervention, n (%)* | Control† | Control, n (%)* | p-value‡ |
|---|---|---|---|---|---|---|
| Studies testing orthotic and/or physical interventions as either a multi-component intervention, or in separate intervention groups | ||||||
| Askoy 2004 Turkey26 |
48 (51) | Orthotics (brace), PT† | 3/23 (13.0) | None, PT† | 6/28 (21.4) | 0.43 |
| Arkader 2008 Brazil27 |
43 (43) | Orthotic (brace), PT (if needed) |
6/21 (28.6) | Surgical | 3/22 (13.6) | 0.23 |
| Herring 2004 USA34 |
337 (345) | Orthotics (brace) | 22/129 (17.1) | None Surgical |
3/19 (15.8) 12/120 (10.0) |
0.89 0.53 |
| PT (ROM) | 16/77 (20.8) | None Surgical |
0.62 0.03 |
|||
| Wang 1995 USA39 |
124 (141) | Orthotics (SRO) | 8/41 (19.5) | Surgical | 6/30 (20.0) | 0.96 |
| PT (NWB exercise)† | 7/41 (17.1) | Surgical | 0.76 | |||
| Petrie cast | 1/41 (2.4) | Surgical | 0.01 | |||
| Wiig 2008 Norway40 |
323 (323) | Orthotics | 13/13 (27.7) | Surgical | 10/93 (10.8) | 0.01 |
| PT | 37/174 (21.3) | Surgical | 0.03 | |||
| Studies testing orthotic interventions only | ||||||
| Citlak 2012 Turkey29 |
25 (27) | Orthotics (Thomas splint) | 2/16 (12.5) | Surgical | 0/11 (0.0) | 0.22 |
| Osman 2009 Scotland37 |
44 (48) | Orthotic (abduction cast) | 3/12 (25.0) | None Surgical |
8/14 (57.1) 2/22 (9.1) |
0.10 |
-
*
Number achieving a Stulberg score of 4 or 5 indicating a poor radiological outcome.
-
†
Two control group tested: no intervention (none) and surgery intervention.
-
‡
p-values calculated by the review team from event rate data extracted from the paper.
-
NWB, non-weightbearing; PT, physiotherapy; ROM, range of movement; SRO, Scottish Rite orthosis.
Table III.
Orthotic interventions: Primary outcome assessed using Mose method.
| Author | Children, hips (n) | Intervention | Intervention, n (%)* | Control† | Control, n (%)* | p-value‡ |
|---|---|---|---|---|---|---|
| Edvarson 1981 Norway31 |
58 (63) | Bed rest/sling | 6/32 (18.8) | Surgical | 7/31 (22.6) | 0.71 |
| Evans 1988 USA32 |
36 (36) | Orthotics (Newton Abduction Orthosis) | 3/17 (17.6) | Surgical | 5/19 (26.3) | 0.53 |
| Osman 2009 Scotland37 |
44 (48) | Orthotic (abduction cast) | 5/12 (42.0) | None Surgical |
11/14 (78.6) 13/22 (59.1) |
0.06 0.34 |
-
*
Number achieving a ‘Poor’ Mose score indicating a poor radiological outcome.
-
†
Two control group tested: no intervention (none) and surgery intervention.
-
‡
p-values calculated by the review team from data presented in the paper.
There were no statistically significant between-group differences in any secondary outcomes (range of movement, gait disturbance, or quality of gait) reported in studies comparing orthotic management to surgery.29,31-33
Studies comparing physical intervention with no intervention or surgery
The primary outcome findings (Stulberg score) for studies comparing physical interventions (such as ROM exercises, or ‘physiotherapy’) with a comparator of no intervention34 or surgical repair39,40) were also inconsistent (Table II). While reporting no between-group differences when comparing physical interventions with no intervention, Wiig et al40 reported a higher proportion of children with poor radiological outcomes among those receiving physiotherapy intervention compared with those undergoing surgery (p < 0.05). In contrast, the proportions of children with poor outcomes were similar in the remaining two studies that provided ROM exercises34 or a multicomponent intervention comprising weight-bearing modification and exercises.39
Regarding secondary outcomes, Brech et al28 studied 17 children (eight physiotherapy, nine no intervention) treated with a physiotherapy regime consisting of stretching, strengthening and balance work compared with those receiving active observation (no details specified). Measures of ROM and strength were greater in the physiotherapy group compared to those receiving no intervention (all p < 0.05).
Relationship between age and treatment effects
Several studies investigated the relationship between the age of intervening and clinical outcomes. In three studies, children treated under the age of 12 years were reported to have improved radiological outcomes when treated with non-surgical intervention (orthotic and physical interventions)30 compared with those aged 12 years or over at the time of intervention (data not presented).37,40 Cooperman et al30 compared two orthotic interventions (Scottish rite orthosis and Newington abduction orthosis) with the use of crutches and surgery. No difference in outcome between the four methods was reported for children under the age of 12 years, although a higher proportion of children over 12 years using crutches had poor Stulberg outcomes when compared to other groups.28 The lateral pillar classification, a radiological assessment of the hip joint used by Herring et al34 indicated that there were no significant differences between children who had surgery and those who underwent physical interventions (ROM exercises) or orthotic management. However, these authors did report that a larger proportion of children were in the favourable Stulberg 1 or 2 category when compared with no treatment (40% overall compared with 26% for no treatment); when adjusted for patients under the age of 8 years old this proportion increased to 48% for ROM exercises.37 Wiig et al40 concluded that in children aged less than six years, physiotherapy resulted in the highest number of children in the favourable Stulberg 1 or 2 category compared to orthotic or surgical intervention. They also reported there was a higher proportion of children with femoral head necrosis (over 50%) aged six years or older.
Discussion
Main findings
In this review, we found no high-quality evidence to suggest that specific types of orthotic management or physical interventions, either alone or in combination, were constituently associated with improved radiological outcomes when compared with alternative treatment strategies. Children achieving poor radiological outcomes ranged from 13% to 42% with orthotic interventions, 17% to 21% for those receiving physical interventions and 0% to 59% for surgical interventions. Although 15 studies met our inclusion criteria, none were randomized controlled trials. Furthermore, the quality of these studies was variable with most being at unknown or high risk of bias. The evidence available was difficult to synthesize due to heterogeneous designs and comparator interventions and limited reporting of treatment protocols for the interventions tested.
While conclusions are limited regarding effectiveness of interventions, a number of studies did reveal interesting differences in treatment response associated with the age of the child at time of diagnosis and intervention. Three studies reported better radiological outcomes associated with both surgical and non-surgical interventions in younger children.28,34,40 Findings reported in the wider existing literature suggest that surgical interventions on the other hand may lead to better outcomes when performed in older children.41,42 These differences in treatment response might be explained by the differing structural changes in those older children (aged > 5/6 years), such as loss of hip joint congruence leading to increased risk of femoral head deformation.41
Findings in context
This is the first systematic review to focus primarily on non-surgical treatments of Perthes’ disease. A previous meta-analysis by Nguyen et al43 analyzed the radiological outcomes of children with Perthes’ disease following surgical intervention, compared with other surgical methods as well as some non-surgical approaches. This review concluded that for children aged under six years, there was no difference in radiological outcomes between different treatment approaches. Those older than six years in this review were all treated surgically, and outcomes appeared similar regardless of surgical technique. Since the completion of this meta-analysis, only one additional publication has been identified that assesses the effectiveness of non-surgical treatment.29
In the UK, a survey of members of BSCOS reported that 90% of clinicians refer children with Perthes’ disease to physiotherapy services.44 One of the aims of treatment delivered in physiotherapy services is to maintain mobility of the hip joint based on evidence, suggesting more favourable outcomes in children with preserved hip ROM.45 Our review has highlighted the limited evidence base for this treatment approach; only four studies27,28,34,40 tested a physical therapy intervention, and the findings were inconclusive.
Study strengths and limitations
This review includes the assessment of 1,805 hips in 1,745 children, who were followed-up for a range of 12 weeks to 33 years. All but two studies26,28 reported follow-up until the point of skeletal maturity, which is important in the management of Perthes’ disease to ensure disease process completion.4
While a major strength of this review is that it summarizes the available evidence on non-surgical treatment options for Perthes’ disease, it is limited by the lack of robust evidence. Another limitation is that it was not possible to pool results for statistical analysis due to the heterogeneity in methodology and in non-surgical interventions evaluated within our broad categories of orthotic or physical management. To aid narrative synthesis, significance levels were calculated to aid the reader’s interpretation of the radiological outcomes; however, as no adjustments for baseline characteristics could be made and these findings should be treated with caution. Finally, it was not possible to explore the impact of interventions upon outcomes likely to be important to children and their families and carers, such as function and health-related quality of life, as the majority of studies limited their reporting to radiological and clinical outcome measures. A core outcome set (COS) for Perthes’ disease has been created, which defines a much wider standardized set of outcomes that are important when measuring the success of interventions.46 The use of this COS will allow standardization in clinical outcomes that can, in turn, support decision making for treatments in this patient population.
This review demonstrates a lack of evidence regarding the effectiveness of treatments for Perthes’ disease, such that no recommendations can be made regarding the use of any non-surgical intervention compared to other non-surgical or surgical interventions. Future research must employ high-quality randomized trials to inform clinical practice. This research should not only include radiological outcomes, but should seek to include patient-important outcomes, such as pain and functional recovery, that make up the COS.
References
1. Loder RT , Skopelja EN . The epidemiology and demographics of Legg-Calvé-Perthes' disease . ISRN Orthop . 2011 ; 2011 : 1 – 14 . Crossref PubMed Google Scholar
2. Margetts BM , Perry CA , Taylor JF , Dangerfield PH . The incidence and distribution of Legg-Calvé-Perthes disease in Liverpool, 1982-95 . Arch Dis Child . 2001 ; 4 : 351 – 354 . Google Scholar
3. Johansson T , Lindblad M , Bladh M , Josefsson A , Sydsjö G . Incidence of Perthes’ disease in children born between 1973 and 1993: A Swedish nationwide cohort study of 2.1 million individuals . Acta orthopaedica . 2017 ; 88 ( 1 ): 96 – 100 . Google Scholar
4. Perry DC . Unravelling the enigma of Perthes disease . Ann R Coll Surg Engl . 2013 ; 95 ( 5 ): 311 – 316 . Crossref PubMed Google Scholar
5. Stulberg SD , Cooperman DR , Wallensten R . The natural history of Legg-Calvé-Perthes disease . J Bone Joint Surg Am . 1981 ; 7 : 1095 – 1108 . PubMed Google Scholar
6. Kim HKW . Legg-Calvé-Perthes disease . J Am Acad Orthop Surg . 2010 ; 11 : 676 – 686 . Crossref PubMed Google Scholar
7. Joseph B , Nair NS , Narasimha Rao KL , Mulpuri K , Varghese G . Optimal timing for containment surgery for Perthes disease . J Pediatr Orthop . 2003 ; 23 ( 5 ): 601 – 606 . Crossref PubMed Google Scholar
8. Brech GC , Guarnieiro R . Evaluation of physiotherapy in the treatment of Legg-Calvé-Perthes disease . Clinics . 2006 ; 6 : 521 – 528 . Crossref PubMed Google Scholar
9. Manig M . Legg-Calvé-Perthes disease (LCPD). principles of diagnosis and treatment . Der Orthopade . 2013 ; 10 : 891 – 904 . Google Scholar
10. Price CT , Thompson GH , Wenger DR . Containment methods for treatment of Legg-Calvé-Perthes disease . Orthop Clin North Am . 2011 ; 3 : 329 – 340 . Crossref PubMed Google Scholar
11. Catterall A . The natural history of Perthes' disease . J Bone Joint Surg Br . 1971 ; 53 ( 1 ): 37 – 53 . Crossref PubMed Google Scholar
12. Rich MM , Schoenecker PL . Management of Legg-Calvé-Perthes disease using an A-frame orthosis and hip range of motion: a 25-year experience . J Pediatr Orthop . 2013 ; 33 ( 2 ): 112 – 119 . Crossref PubMed Google Scholar
13. Alliance JL . Priority 4 from the paediatric lower limb surgery PSP . 2020 . http://www.jla.nihr.ac.uk/priority-setting-partnerships/Paediatric-lower-limb-surgery/priority-4-from-the-paediatric-lower-limb-surgery-psp.htm (date last accessed 29 October 2020 ). Google Scholar
14. Vella-Baldacchino M , Perry DC , Roposch A , et al. Research priorities in children requiring elective surgery for conditions affecting the lower limbs: a James Lind alliance priority setting partnership . BMJ Open . 2019 ; 9 ( 12 ): e033233 – 033235 . Crossref PubMed Google Scholar
15. Perry DC , Wright JG , Cooke S , et al. A consensus exercise identifying priorities for research into clinical effectiveness among children's orthopaedic surgeons in the United Kingdom . Bone Joint J . 2018 ; 100-B ( 5 ): 680 – 684 . Crossref PubMed Google Scholar
16. Galloway AM , van Hille T , Perry D , et al. Non-Surgical management of Perthes disease in children. Prospero . 2019 . https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42019141589 (date last accessed 29 October 2020 ). Google Scholar
17. Mose K . Methods of measuring in Legg-Calvé-Perthes disease with special regard to the prognosis . Clin Orthop Relat Res . 1980 ; 150 : 103 – 109 . PubMed Google Scholar
18. O’Brien M . Aids to the examination of the peripheral nervous system . 5th edn . London : Saunders, Elsevier , 2010 . Google Scholar
19. Cochrane Effective Practice and Organisation of Care (EPOC) . Epoc resources for review authors . 2017 . epoc.cochrane.org/resources/epoc-resources-review-authors (date last accessed 29 October 2020 ). Google Scholar
20. Wells GA , Shea B , O'Connell D , et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses . 2019 . www.ohri.ca/programs/clinical_epidemiology/oxford.asp (date last accessed 29 October 2020 ). Google Scholar
21. Li W , Ma D , Liu M , et al. Association between metabolic syndrome and risk of stroke: a meta-analysis of cohort studies . Cerebrovasc Dis . 2008 ; 25 ( 6 ): 539 – 547 . Crossref PubMed Google Scholar
22. Veronese N , Cereda E , Solmi M , et al. Inverse relationship between body mass index and mortality in older nursing home residents: a meta-analysis of 19,538 elderly subjects . Obes Rev . 2015 ; 16 ( 11 ): 1001 – 1015 . Crossref PubMed Google Scholar
23. Hoffmann TC , Glasziou PP , Boutron I , et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide . BMJ . 2014 ; 348 : g1687 . Crossref PubMed Google Scholar
24. Yamato TP , Maher CG , Saragiotto BT , Catley MJ , Moseley AM . Rasch analysis suggested that items from the template for intervention description and replication (TIDieR) checklist can be summed to create a score . J Clin Epidemiol . 2018 ; 101 : 28 – 34 . Google Scholar
25. Moher D , Liberati A , Tetzlaff J , Altman DG , The PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement . BMJ . 2009 ; 2009 ( 339 ): b2535 . Crossref PubMed Google Scholar
26. Aksoy MC , Caglar O , Yazici M , Alpaslan AM . Comparison between braced and non-braced Legg-Calvé-Perthes-disease patients: a radiological outcome study . J Pediatr Orthop B . 2004 ; 13 ( 3 ): 153 – 157 . Crossref PubMed Google Scholar
27. Arkader A , Sankar WN , Amorim RM . Conservative versus surgical treatment of late-onset Legg-Calve-Perthes disease: a radiographic comparison at skeletal maturity . J Child Orthop . 2009 ; 3 ( 1 ): 21 – 25 . Crossref PubMed Google Scholar
28. Brech GC , Guarnieiro R . Evaluation of physiotherapy in the treatment of Legg-Calvé-Perthes disease . Clinics . 2006 ; 61 ( 6 ): 521 – 528 . Crossref PubMed Google Scholar
29. Cıtlak A , Kerimoğlu S , Baki C , Aydın H . Comparison between conservative and surgical treatment in Perthes disease . Arch Orthop Trauma Surg . 2012 ; 132 ( 1 ): 87 – 92 . Crossref PubMed Google Scholar
30. Cooperman DR , Stulberg SD . Ambulatory containment treatment in Perthes?? disease . Clin Orthop Relat Res . 1986 ; &NA ( 203 ): 289 – 300 . Google Scholar
31. Edvardsen P , Slørdahl J , Svenningsen S . Operative versus conservative treatment of Calvé-Legg-Perthes disease . Acta Orthop Scand . 1981 ; 52 ( 5 ): 553 – 559 . Crossref PubMed Google Scholar
32. Evans IK , Deluca PA , Gage JR . A comparative study of ambulation-abduction bracing and varus derotation osteotomy in the treatment of severe Legg-Calvé-Perthes disease in children over 6 years of age . J Pediatr Orthop . 1988 ; 8 ( 6 ): 676 – 682 . Crossref PubMed Google Scholar
33. Fulford GE , Lunn PG , Macnicol MF . A prospective study of nonoperative and operative management for Perthes' disease . J Pediatr Orthop . 1993 ; 13 ( 3 ): 281 – 285 . Crossref PubMed Google Scholar
34. Herring JA , Kim HT , Browne R , Disease L-C-P . Legg-Calve-Perthes disease. Part II: prospective multicenter study of the effect of treatment on outcome . J Bone Joint Surg Am . 2004 ; 86 ( 10 ): 2121 – 2134 . PubMed Google Scholar
35. Jani L , Dick W . Results of three different therapeutic groups in Perthes' disease . Clin Orthop Relat Re . 1980 ; 150 : 88 – 94 . PubMed Google Scholar
36. Marklund T , Tillberg B . Primary results of conservative treatment and osteotomy in Coxa plana: a radiological comparison . Clin Orthop Relat Res . 1977 ; 127 : 142 – 147 . PubMed Google Scholar
37. Osman MK , Martin DJ , Sherlock DA . Outcome of late-onset Perthes' disease using four different treatment modalities . J Child Orthop . 2009 ; 3 : 235 – 242 . Crossref PubMed Google Scholar
38. Poussa M , Yrjönen T , Hoikka V , Osterman K . Prognosis after conservative and operative treatment in Perthes' disease . Clin Orthop Relat Res . 1993 ; 297 : 82 – 86 . PubMed Google Scholar
39. Wang L , Bowen R , Puniak MA , Guille JT , Glutting J . An evaluation of various methods of treatment for Legg-Calve-Perthes disease . Clin Orthop Relat Res . 1995 ; 314 : 225 – 233 . Google Scholar
40. Wiig O , Terjesen T , Svenningsen S . Prognostic factors and outcome of treatment in Perthes' disease . J Bone Joint Surg Br . 2008 ; 90 ( 8 ): 1364 – 1371 . Crossref PubMed Google Scholar
41. Joseph B . Management of Perthes' disease . Indian J Orthop . 2015 ; 49 ( 1 ): 10 – 16 . Crossref PubMed Google Scholar
42. Canavese F , Dimeglio A Perthes' disease: prognosis in children under six years of age . Bone Joint Surg Br . 2008 ; 90 ( 7 ): 940 – 945 . Crossref PubMed Google Scholar
43. Nguyen N-AT , Klein G , Dogbey G , McCourt JB , Mehlman CT . Operative versus nonoperative treatments for Legg-Calvé-Perthes disease: a meta-analysis . J Pediatr Orthop . 2012 ; 32 ( 7 ): 697 – 705 . Crossref PubMed Google Scholar
44. Annamalai SKM , Buckingham R , Cashman J . Perthes disease: a survey of management amongst members of the British Society for children's orthopaedic surgery (BSCOS) . J Child Orthop . 2007 ; 1 ( 2 ): 107 – 113 . Crossref PubMed Google Scholar
45. Stanitski CL . Hip range of motion in Perthes' disease: comparison of pre-operative and intra-operative values . J Child Orthop . 2007 ; 1 ( 1 ): 33 – 35 . Crossref PubMed Google Scholar
46. Leo DG , Jones H , Murphy R , et al. The outcomes of Perthes' disease . Bone Joint J . 2020 ; 102-B ( 5 ): 611 – 617 . Crossref PubMed Google Scholar
Author contributions
A. M. Galloway: Designed the study, Collected and analyzed the data, Prepared and reviewed the manuscript.
T. van-Hille: Collected and analyzed the data, Reviewed the manuscript.
D. C. Perry: Designed the study, Prepared and reviewed the manuscript.
C. Holton: Designed the study, Prepared and reviewed the manuscript.
L. Mason: Designed the study, Collected the data, Reviewed the manuscript.
S. Richards: Designed the study, Analyzed the data, Prepared and reviewed the manuscript.
H. J. Siddle: Designed the study, Analyzed the data, Prepared and reviewed the manuscript.
C. Comer: Designed the study, Analyzed the data, Prepared and reviewed the manuscript.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Acknowledgements
A. Galloway is funded by a National Institute for Health Research (NIHR) and Health Education England (HEE) Pre-doctoral Clinical Academic Fellowship. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Follow A. M. Galloway @GallowayAdam
Follow T. van-Hille @TomvanHillePT
Follow D. C. Perry @MrDanPerry
Follow C. Holton @HoltonColin
Follow S. Richards @RichaSuzy
Follow H. J. Siddle @HeidiSiddle
Follow C. Comer @DrCComer
Supplementary material
Tables showing the detailed Newcastle Ottawa Score and TIDieR checklist.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited. See https://creativecommons.org/licenses/by-nc-nd/4.0/.
