




Abstract
Aims
Mobile-bearing unicompartmental knee arthroplasty (UKA) with a flat tibial plateau has not performed well in the lateral compartment, leading to a high rate of dislocation. For this reason, the Domed Lateral UKA with a biconcave bearing was developed. However, medial and lateral tibial plateaus have asymmetric anatomical geometries, with a slightly dished medial and a convex lateral plateau. Therefore, the aim of this study was to evaluate the extent at which the normal knee kinematics were restored with different tibial insert designs using computational simulation.
Methods
We developed three different tibial inserts having flat, conforming, and anatomy-mimetic superior surfaces, whereas the inferior surface in all was designed to be concave to prevent dislocation. Kinematics from four male subjects and one female subject were compared under deep knee bend activity.
Results
The conforming design showed significantly different kinematics in femoral rollback and internal rotation compared to that of the intact knee. The flat design showed significantly different kinematics in femoral rotation during high flexion. The anatomy-mimetic design preserved normal knee kinematics in femoral rollback and internal rotation.
Conclusion
The anatomy-mimetic design in lateral mobile UKA demonstrated restoration of normal knee kinematics. Such design may allow achievement of the long sought normal knee characteristics post-lateral mobile UKA. However, further in vivo and clinical studies are required to determine whether this design can truly achieve a more normal feeling of the knee and improved patient satisfaction.
Cite this article: Bone Joint Res 2020;9(7):421–428.
Article focus
-
The influence of lateral tibial insert designs on knee kinematics in mobile-bearing unicompartmental knee arthroplasty (UKA).
Key message
-
The anatomy-mimetic lateral mobile UKA design has shown more proper kinematics in femoral rollback and internal rotation than that of the flat and conforming designs.
Strength and limitations
-
This study showed that the surface design of the tibial lateral insert has a significant impact on the restoration of normal knee kinematics in mobile-bearing UKA.
-
The model used in this study assumes the material properties and attachment points of the ligaments based on highly variable values from the reference.
Introduction
Most of the published results addressing unicompartmental knee arthroplasty (UKA) relate to the medial compartment.1,2 UKA is an appropriate procedure for patients with unilateral knee osteoarthritis. While the reported results of medial UKA have been comparable to those of total knee arthroplasty (TKA),2-4 the results of lateral UKA are still controversial,5,6 likely because indications for this procedure are still not well established, particularly for the lateral compartment. In addition, lateral UKA is technically more challenging than medial UKA, due to difficulties with exposure, as well as the shortcomings of traditional unicompartmental implants that do not take into consideration the anatomical differences between the medial and lateral compartments. There are potential advantages to both mobile and fixed bearings in this situation. Mobile bearings have the advantage in terms of the polyethylene wear and better improved kinematics compared to fixed-bearing designs.7-9 This could be a particular advantage in the lateral compartment, where there is a large amount of femoral rollback in flexion.10 Despite these theoretical advantages, the results for mobile bearing designs in the lateral compartment have been less encouraging, with a 10% rate of dislocation reported in the first year.11 Therefore, modification in the surgical technique and adaptation of the implant design to a domed tibial component and biconcave tibial insert will potentially allow the use of a mobile-bearing insert in the lateral compartment.12,13
Typically, the medial and lateral tibial plateaus have asymmetric geometries, with a slightly dished medial plateau and a convex lateral plateau.14,15 In addition, the screw home mechanism is much more significant on the lateral side. The dished medial plateau and the greater stability of the medial meniscus restrict the anteroposterior (AP) translation and posterior rollback of the medial femoral condyle. In contrast, the convex lateral plateau combined with the lateral meniscus mobility shows greater range of AP motion with greater posterior rollback of the lateral femoral condyle.16 This patient-specific design may improve the biomechanical behaviour of lateral UKA as it may provide more natural biomechanics.17
However, the current patient-specific UKA inserts have been designed with fixed bearing. As previously mentioned, the lateral plateau has greater mobile characteristics than the medial plateau. In addition, one of the potential limitations of a completely patient-specific design is the variability in coronal curvature of the femoral component, which may cause point loading in particular flexion angles when a curved tibial insert is used. To address this problem, a flat tibial insert should be used with the constant coronal curvature femoral component, which ensures constant loading in a large area irrespective of the flexion angle.18 A recent study showed that reduction in tibiofemoral conformity preserved natural knee kinematics in patient-specific lateral UKA.19 However, their study disregarded mobile characteristics in lateral tibial plateau.19
Therefore, the aim of this study was to evaluate the extent to which the normal knee kinematics was restored with different tibial insert designs using computational simulation. We developed three different tibial inserts having flat, conforming, and anatomy-mimetic superior surfaces, and the inferior surface in all was designed to be concave to prevent dislocation. We hypothesized that the anatomy-mimetic design preserves the closest kinematics to that of normal knee in lateral UKA.
Methods
Design of mobile patient-specific inserts for lateral UKA
This study was approved by our hospital’s Institutional Review Board and written informed consent was obtained from each subject. Four male subjects (Subject 1: age 36 years, height 178 cm, mass 75 kg; Subject 2: age 34 years, height 173 cm, mass 83 kg; Subject 3: age 32 years, height 182 cm, mass 79 kg; Subject 4: age 34 years, height 173 cm, mass 71 kg) and one female subject (Subject 5: age 26 years, height 163 cm, mass 65 kg) without any medical history of knee joint problems participated in this study. The patient-specific lateral UKA insert was designed using a previously existing 3D knee joint model.20-22 CT and MRI scans were initially performed. The image data were imported into Mimics version 14.1 (Materialise, Leuven, Belgium) for 3D reconstruction. Planes were defined through the intersection of condyles in both the sagittal and coronal views. The patient’s bone defines the sagittal geometry of the femoral component. Thus, the sagittal geometry is completely patient-specific; the resultant sagittal implant radii vary with respect to the AP dimension of the implant (Figure 1). The coronal curvatures of the patient are measured at multiple positions along the length of the femoral condyle, and a mean curvature is evaluated using this data for each patient.23 In this approach, a patient-derived constant coronal curvature is achieved.23 The tibial component is designed using the CT and MRI data of the patient’s tibia to ensure complete cortical rim coverage. However, unlike femoral components, three different tibial insert designs were applied. They were the flat design, anatomy-mimetic convex design, and conformity-increasing design (Figure 2). This method was used for all subject-specific models. In addition, the inferior surface was designed to be concave to prevent dislocation of mobile bearing.
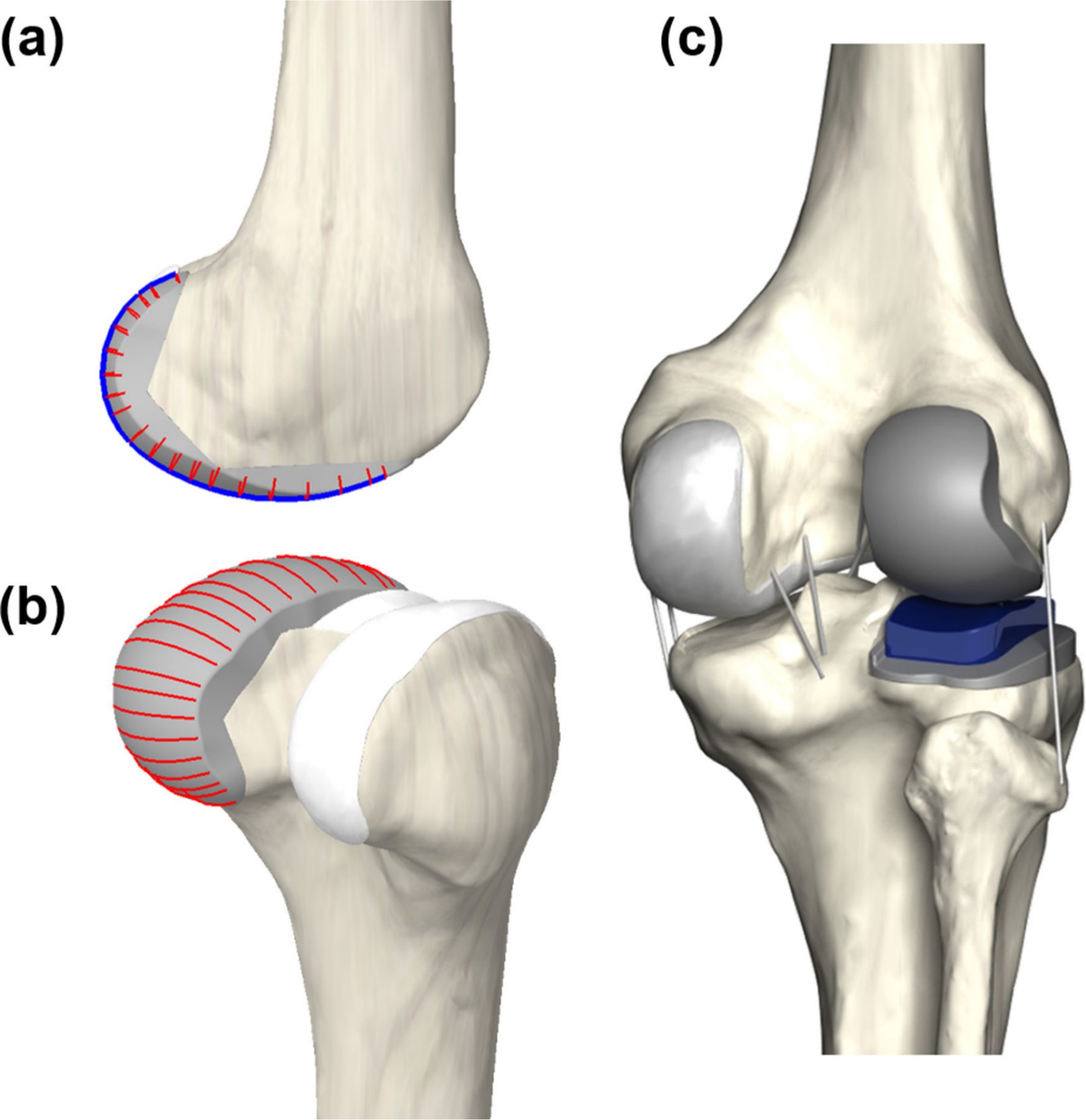
Fig. 1
Design process of patient-specific unicompartmental knee: a) spline curves used to model the femoral component; b) polyethylene insert that provides an anatomical fit and a perfect coverage; and c) patient-specific unicompartmental knee arthroplasty (UKA) model design.
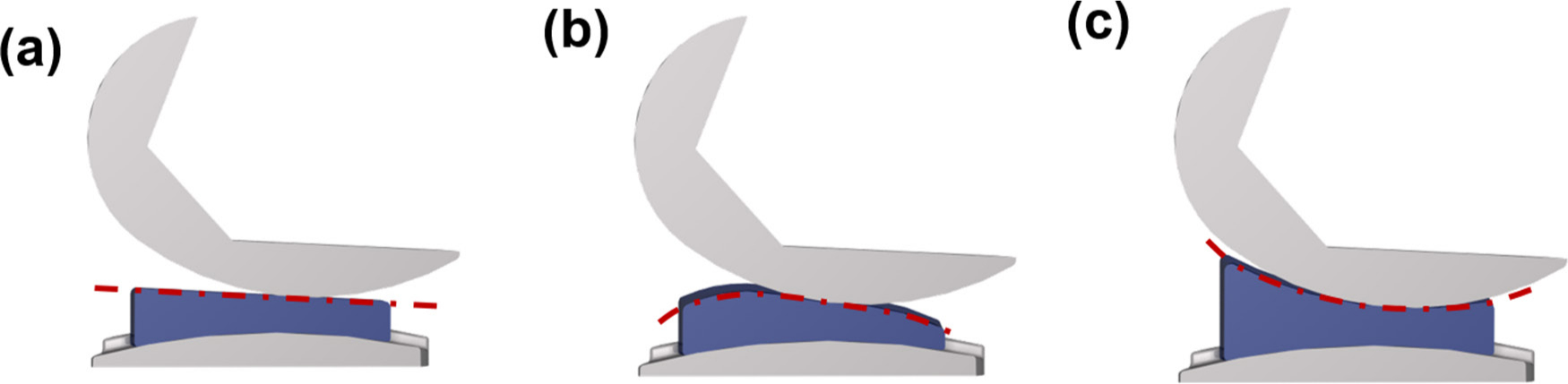
Fig. 2
The three different FE models used in the analysis: a) flat design; b) anatomy-mimetic convex design; and c) conformity design.
Development of patient-specific finite element model for lateral mobile UKA
The previously mentioned 3D medical imaging data used for a patient-specific lateral mobile UKA development were used in the development of the finite element (FE) model (Figure 2).20-23 3D bone and soft tissue models were reconstructed from CT and MRI, as described in previous studies.18,23,24 All the ligament bundles were modelled as non-linear springs, and the material properties were obtained from previous studies.25,26 The heights of the tibial insert for the three different designs were matched to the original bone anatomy using a sagittal cross-sectional image, then aligned with the mechanical axis and positioned at the medial edge with a square (0°) inclination in the coronal plane of the tibia.25 The rotating axis was defined as the line parallel to the lateral edge of the tibial baseplate passing through the centre of the femoral component fixation peg. For the implanted model, a 1 mm cement gap was considered between the component and bone. Material properties of the femoral component, tibial insert, tibial baseplate, and bone cement are referred to in previous studies (Table I).19,23-29
Table I.
Material properies for finite element model.
| Variable | Young’s modulus (MPa) | Poisson’s ratio |
|---|---|---|
| CoCr alloy | 220,000 | 0.30 |
| UHMWPE | 685 | 0.47 |
| Ti6AI4V alloy | 110,000 | 0.30 |
| PMMA | 1,940 | 0.4 |
-
PMMA, polymethyl methacrylate; UHMWPE, ultra-high-molecular-weight polyethylene.
Loading and boundary conditions
This FE simulation included two types of loading conditions, corresponding to the loads used in the experiment for model validation and predictions for daily activity loading scenarios. Under the first loading condition, 1,150 N was applied to the model to obtain the contact stresses and compare them to those reported in a published FE knee joint study.30 The second loading condition, corresponding to the deep knee bend loading, was applied to evaluate the knee joint mechanics. A computational analysis was performed using an AP force applied to the femur with respect to the compressive load applied to the hip with a constrained femoral internal-external (IE) rotation, free medial-lateral translation, and knee flexion determined through a combination of the vertical hip and the load of the quadriceps. Thus, a six degree-of-freedom tibiofibular joint was created.31,32 A proportional-integral-derivative controller was incorporated into the computational model to control the quadriceps in a manner similar to that used in a previous experiment.20 A control system was used to evaluate the instantaneous displacement of the quadriceps muscle, which was required to match the same target flexion profile as that in the experiment. IE and varus-valgus torques were applied to the tibia, while the remaining tibial degrees-of-freedom were constrained.31,32 The FE model was simulated using ABAQUS software (version 6.11; Simulia, Providence, Rhode Island, USA). This study investigated and compared the kinematics of patient-specific UKA designs with three different conformities derived from a normal knee. The kinematics were calculated based on Grood and Suntay’s definition of a joint coordinate system.33 This research has been approved by the IRB of the authors’ affiliated institutions (Institutional Review Board Protocol Number FINITE ELEMENT ANALYSIS 2.0).
Statistical analysis
Single cycles of deep knee bend loading condition were divided into 11 timepoints (0.0 to 1.0 phases). To assess the three different tibial insert designs - flat, anatomy-mimetic, and conforming - each design’s condition was compared to the normal knee in pairwise manner using non-parametric repeated-measure Friedman tests at each phase of the cycle. The post-hoc comparisons were performed using a Wilcoxon's rank test with Holm correction, to control the familywise error rate for the tests conducted within each phase of the cycle. Statistical analyses were performed using SPSS for Windows (version 20.0.0; IBM, Armonk, New York, USA). Statistical significance was set at p < 0.05 for all comparisons.
Results
Normal knee validation
The five-subject-specific FE model was validated by comparison with the previous study. The mean contact stresses of 3.1 MPa (SD 0.4) and 1.53 MPa (SD 0.6) were evaluated on the medial and lateral meniscus, respectively, under an axial load of 1,150 N. For both medial and lateral menisci, the result from the previous study was within the ranges of mean contact stress in our study.30 These differences may be caused by geometrical variations between these studies, such as the thickness of the cartilage and meniscus. The considerable consistency between the validation results and the results from the literature showed the validity of the results obtained through the FE model used in this study.
Comparison of kinematics in patient-specific lateral mobile UKA designs for three different conformities and normal knee under deep knee bend
Figure 3 shows the femoral rollback of the three patient-specific lateral mobile designs and that of a normal knee under deep knee bend. Normal knee under deep knee bend showed an increase in femoral rollback with flexion. The mobile lateral UKA designs also displayed this characteristic of the normal knee on the computational simulation, with values in the same range. However, the flat mobile UKA design showed significantly greater femoral rollback than the normal knee. In contrast, the conforming mobile UKA design showed significantly less femoral rollback than the normal knee. Interestingly, the anatomy-mimetic mobile bearing UKA showed the femoral rollback closest to that of the normal knee.
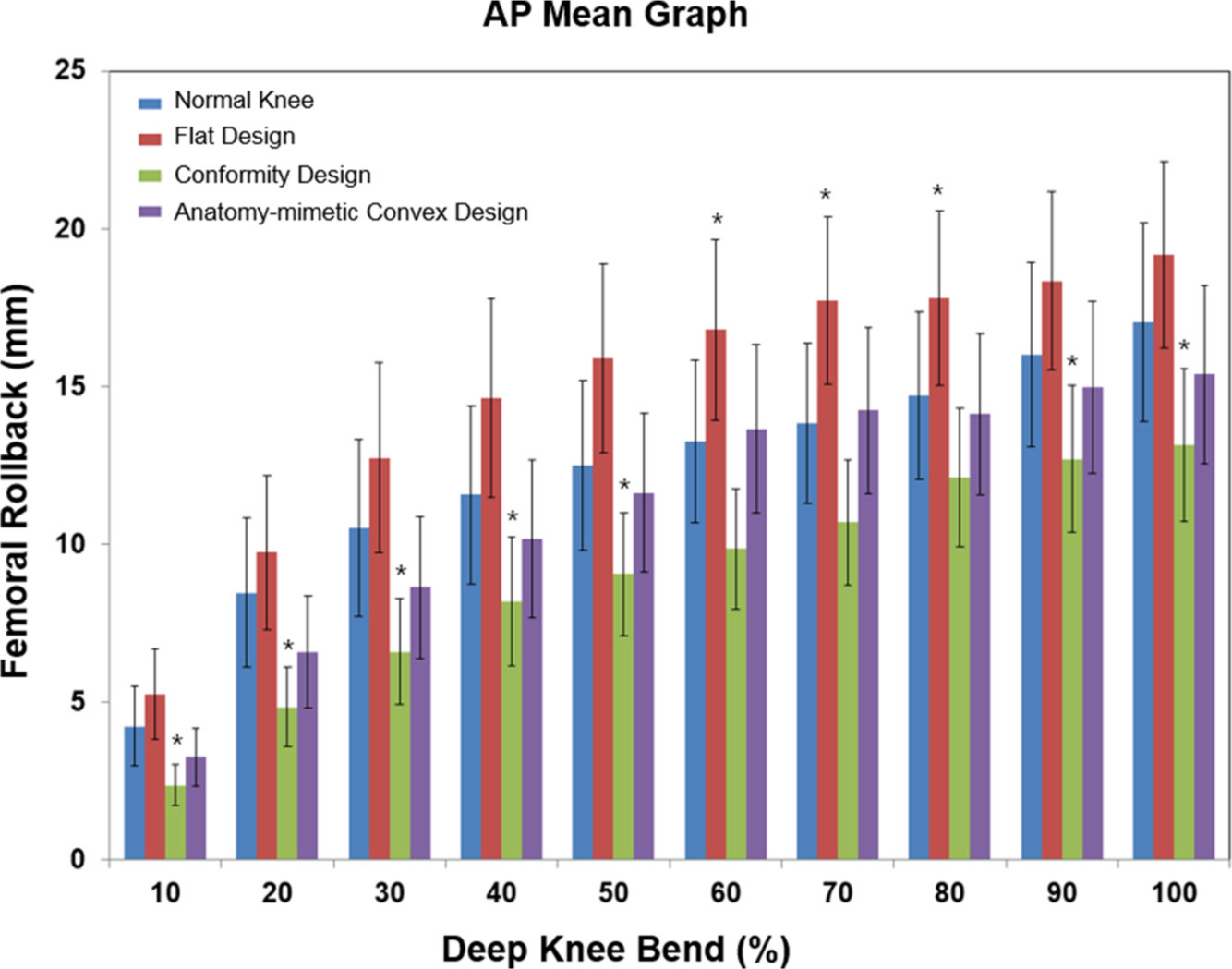
Fig. 3
Comparison of mean (SD) of the femoral rollback for three different unicompartmental knee arthroplasty (UKA) designs under deep knee bend. *p < 0.05. AP, anteroposterior.
Figure 4 shows the tibial internal rotation of the three patient-specific lateral mobile designs and that of the normal knee under deep knee bend. In different activities, normal knees showed rapid increase in tibial internal rotation from 0° to 30° flexion with a range of 6.3° to 12.8° that is consistent with the ‘screw home’ motion. The anatomy-mimetic mobile UKA design showed the screw home motion of the knee between 0° and 30° flexion with the same range. From mid to high flexion, normal knees continued to show a gradually increased tibial rotation. In this flexion range, conforming mobile lateral UKA design showed significantly decreased tibial rotation, although it maintained a net internal rotation of the tibial position. In contrast, the flat mobile lateral UKA design showed significantly greater tibial rotation than the normal knee.
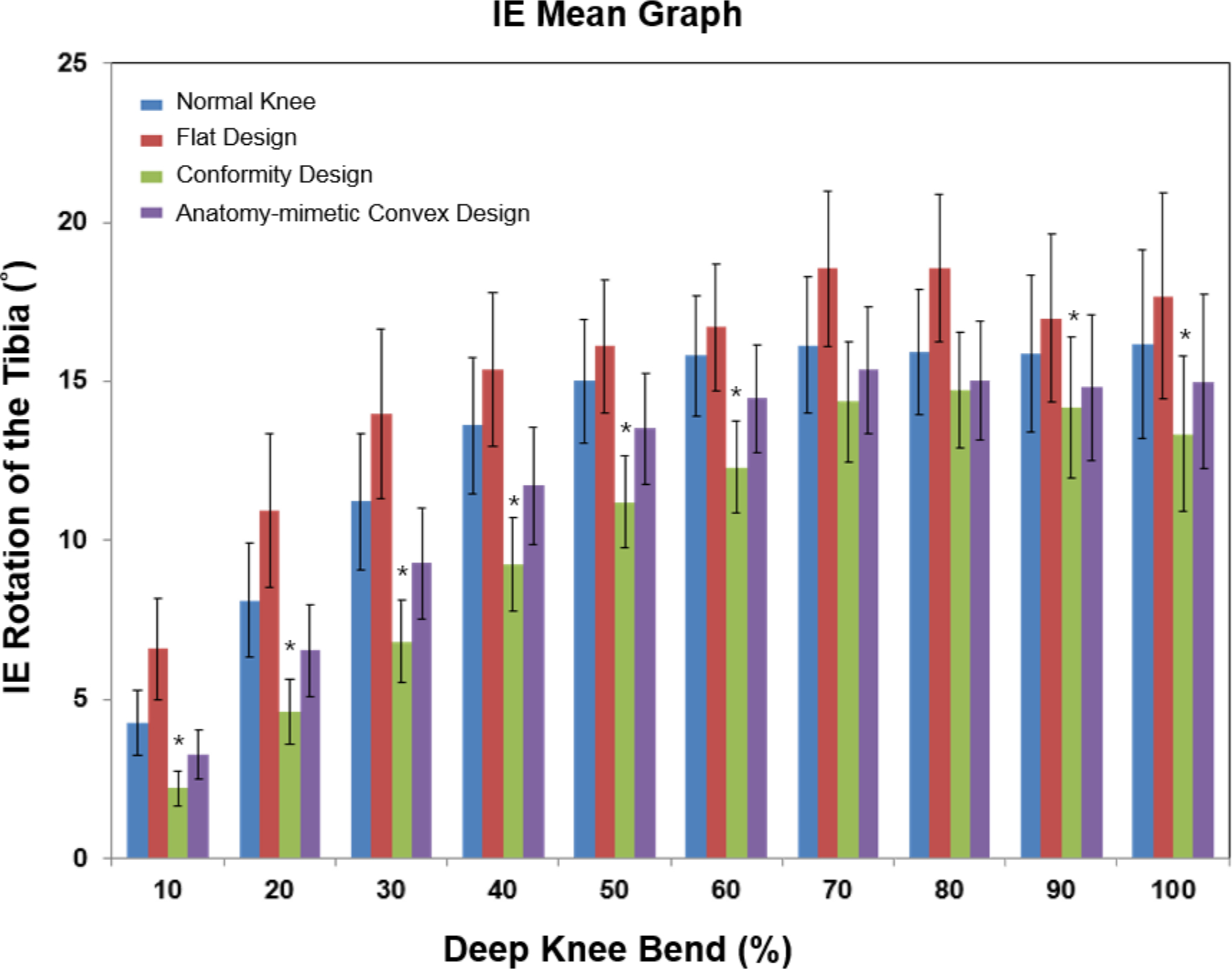
Fig. 4
Comparison of mean (SD) of the tibia internal rotation for three different unicompartmental knee arthroplasty (UKA) designs under deep knee bend. *p < 0.05. IE, internal-external.
Discussion
The most important finding of this study was that the anatomy-mimetic lateral mobile UKA design showed kinematics closest to that of the normal knee. Our result highlighted the importance of the conservation of the tibiofemoral conformity by preservation of patient's anatomy.
A previous study showed that patient-specific lateral UKA designs could provide a successful clinical outcome, as observed postoperatively with the American Knee Society score,34 range of movement, and coronal leg alignment.17 In a previous study, they showed that patient-specific UKA designs provided mechanics closer to that of the normal knee joint.23 The decreased contact stress on the opposite compartment may reduce the overall risk of progressive osteoarthritis.23 As previously mentioned, the lateral tibial condyle is convex, whereas the medial condyle is concave. It means that in deep flexion the medial femoral condyle lies over the tibia. In contrast, the lateral femoral condyle subluxes posteriorly and inferiorly off the back of the tibial plateau as it rotates externally relative to the tibia.35 Thus, in activities of high flexion such as deep knee bend, the knee shows an overall medial pivot motion with greater rollback of the lateral femoral condyle.36,37 However, it is also important to note that the medial tibia does not fully constrain the medial femoral condyle. Consequently, during activities of limited flexion, such as stair-ascending, the AP motion of the medial condyle can be similar to that of the lateral condyle, although the knee shows an overall medial pivot over its full range of movement.38,39 To address the kinematic limitations of contemporary implants, a novel design process was developed to create anatomy-mimetic articular surfaces directly based on in vivo motion of normal knees.16,40,41 However, as previously mentioned, the most serious problem in mobile lateral UKA is dislocation.
Recently, a new mobile bearing lateral UKA design has been developed by using a convex tibial plateau and a biconcave tibial insert (Oxford Domed Lateral Partial Knee; Biomet UK, Bridgend, UK). The initial results of this lateral UKA design demonstrated a better clinical outcome and a reduced dislocation rate of 1.7% versus 11% in the original series with the standard mobile insert.12
Moreover, Altuntas et al42 in a recent study observed that there were no bearing dislocations. Although these are early results, the highest rate of reported dislocations was found within the first two years of surgery; therefore, primary dislocation may be unlikely after this period.12 It was concluded that the domed tibia mobile bearing lateral UKA design supports the safety and efficacy of the procedure as a treatment option in patients with lateral compartment osteoarthritis of the knee.42
Therefore, inferior surface was designed to be concave in this study, to prevent bearing dislocation. The results showed that the femoral rollback and internal rotation kinematics of the native knee were not restored in the flat and conforming mobile lateral UKA designs; however, they were preserved in the anatomy-mimetic mobile lateral UKA design. Flat and conforming designs showed greater and less kinematics in femoral rollback and internal rotation, respectively, than that of the normal knee. This supports the importance of tibiofemoral conformity. The classic 'screw-home' mechanism was reported as a sharp internal rotation near extension,43 and another study showed that the screw-home mechanism is coupled to internal tibial rotation as the femur flexes, and to external tibial rotation as it extends.44 In the present study, the internal rotation angles of the tibia in early flexion in the flat and conforming mobile lateral UKA designs were significantly different from those of the normal knee, indicating that the screw-home mechanism of the normal knee was not restored in these designs; however, it was restored in the anatomy-mimetic mobile lateral UKA design. Whether UKA can restore the kinematics of the normal knee has been the subject of controversy. A previous study investigated six cadaveric human knees using a kinematic rig before and after medial UKA, and reported no significant difference in axial tibial rotation between the normal knee and the flat-surfaced, fixed-bearing UKA knee.45 However, they found that the tibia rotated internally in extension in both normal and UKA knees. For the screw-home mechanism, that finding indicates that the normal knee kinematics were not preserved in UKA. The screw-home mechanism has been attributed to the function of the anterior cruciate ligament and the asymmetry between the medial and lateral femoral condyles.
A previous study suggested that the workings of the screw-home mechanism involved the medial femoral condyle slipping or sliding against the upslope of the tibia as the knee extends, while the lateral femoral condyle suffers no interference as a result of the flattening of the downward sloping anterior part of the lateral tibial condyle.46 In terms of the articular surface, the loss of the upslope of the tibia in the flat-surfaced, fixed-bearing type of UKA caused the changes in rotational kinematics, especially in the early flexion phase. Several previous studies suggested that tibial surface geometry has a considerable impact on the knee joint kinematics.16,40,41 A recent cadaveric study showed that the normal kinematics are lost from the tibial component in bicruciate-retaining TKA, and it suggested that the surface geometry of the tibial insert is an important factor in the restoration of normal rotational kinematics.47
From biomechanical and clinical points of view, the present study confirms the importance of preserving normal geometry for restoration of the kinematics of the normal knee. This important finding implies consideration of the articular surface in knee arthroplasty. In other words, not only is tibial plateau geometry different, but so is medial and lateral tibiofemoral conformity. Therefore, different medial and lateral conformity should be considered in UKA design. Moreover, there are more strong mobile characteristics in lateral tibial plateau than in medial tibial plateau. Therefore, preservation of such a characteristic is important in UKA design with prevention of dislocation.
However, even when knee arthroplasty was performed with an anatomy-mimetic design, perfect normal kinematics could not be restored. The major cause can be considered the difference in material properties between the insert and the soft tissue. To preserve perfect normal knee kinematics, not only design development but material should also be studied further.
Two strengths of the present study should be highlighted. First, in contrast to the current biomechanical UKA model, this study included the deep knee bend loading, as opposed to a simple vertical static loading condition. Second, the biomechanical effect was evaluated using a single model in the previous FE model; however, we developed five subject-specific FE models with different patient-specific tibial insert designs for UKA to investigate their biomechanical effects.
Nevertheless, the current study has three limitations. First, the UKA had fully bonded, and micromotion, which may occur between the tibial compartment and tibial insert, was not considered in this study. Second, we only validated the initial model. However, this method has been widely used in biomechanics. Third, the model assumes the material properties and attachment points of the ligaments based on highly variable values from the reference. However, our objective was not to determine the actual values for muscle and ligament forces, but rather to determine the effect of variability in lateral patient-specific UKA designs with respect to tibial insert conformity for the variables of interest.
In conclusion, the anatomy-mimetic design in lateral mobile UKA demonstrated restoration of normal knee kinematics. Such designs may allow the achievement of the long sought normal knee characteristics post-lateral mobile UKA. However, further in vivo and clinical studies are required to determine whether such anatomy-mimetic design can truly achieve a more normal feeling of the knee and improved patient satisfaction.
References
1. Murray DW , Goodfellow JW , O'Connor JJ . The Oxford medial unicompartmental arthroplasty: a ten-year survival study . J Bone Joint Surg Br . 1998 ; 80-B ( 6 ): 983 – 989 . Crossref PubMed Google Scholar
2. Deshmukh RV , Scott RD . Unicompartmental knee arthroplasty: long-term results . Clin Orthop Relat Res . 2001 ; 392 : 272 – 278 . PubMed Google Scholar
3. Forster MC , Bauze AJ , Keene GC . Lateral unicompartmental knee replacement: fixed or mobile bearing? Knee Surg Sports Traumatol Arthrosc . 2007 ; 15 ( 9 ): 1107 – 1111 . Google Scholar
4. Campi S , Mellon SJ , Ridley D , et al. Optimal interference of the tibial component of the cementless Oxford Unicompartmental Knee Replacement . Bone Joint Res . 2018 ; 7 ( 3 ): 226 – 231 . Crossref PubMed Google Scholar
5. Ohdera T , Tokunaga J , Kobayashi A . Unicompartmental knee arthroplasty for lateral gonarthrosis: midterm results . J Arthroplasty . 2001 ; 16 ( 2 ): 196 – 200 . Crossref PubMed Google Scholar
6. Ashraf T , Newman JH , Evans RL , Ackroyd CE . Lateral unicompartmental knee replacement survivorship and clinical experience over 21 years . J Bone Joint Surg Br . 2002 ; 84-B ( 8 ): 1126 – 1130 . Crossref PubMed Google Scholar
7. Emerson RH , Higgins LL . Unicompartmental knee arthroplasty with the oxford prosthesis in patients with medial compartment arthritis . J Bone Joint Surg Am . 2008 ; 90-A ( 1 ): 118 – 122 . Crossref PubMed Google Scholar
8. Kendrick BJL , Longino D , Pandit H , et al. Polyethylene wear in Oxford unicompartmental knee replacement: a retrieval study of 47 bearings . J Bone Joint Surg Br . 2010 ; 92-B ( 3 ): 367 – 373 . Crossref PubMed Google Scholar
9. Mohammad HR , Campi S , Kennedy JA , et al. Long-term in vivo wear of different bearing types used for the Oxford Unicompartmental Knee Replacement . Bone Joint Res . 2019 ; 8 ( 11 ): 535 – 543 . Crossref PubMed Google Scholar
10. Pinskerova V , Johal P , Nakagawa S , et al. Does the femur roll-back with flexion? J Bone Joint Surg Br . 2004 ; 86-B ( 6 ): 925 – 931 . Crossref PubMed Google Scholar
11. Robinson BJ , Rees JL , Price AJ , et al. Dislocation of the bearing of the Oxford lateral unicompartmental arthroplasty . A radiological assessment. J Bone Joint Surg Br . 2002 ; 84-B ( 5 ): 653 – 657 . Crossref PubMed Google Scholar
12. Pandit H , Jenkins C , Beard DJ , et al. Mobile bearing dislocation in lateral unicompartmental knee replacement . Knee . 2010 ; 17 ( 6 ): 392 – 397 . Crossref PubMed Google Scholar
13. Kayani B , Haddad FS . Robotic unicompartmental knee arthroplasty: Current challenges and future perspectives . Bone Joint Res . 2019 ; 8 ( 6 ): 228 – 231 . Crossref PubMed Google Scholar
14. Fitzpatrick C , FitzPatrick D , Lee J , Auger D . Statistical design of unicompartmental tibial implants and comparison with current devices . Knee . 2007 ; 14 ( 2 ): 138 – 144 . Crossref PubMed Google Scholar
15. Gulati A , Chau R , Beard DJ , et al. Localization of the full-thickness cartilage lesions in medial and lateral unicompartmental knee osteoarthritis . J Orthop Res . 2009 ; 27 ( 10 ): 1339 – 1346 . Crossref PubMed Google Scholar
16. Varadarajan KM , Zumbrunn T , Rubash HE , et al. Cruciate retaining implant with biomimetic articular surface to reproduce activity dependent kinematics of the normal knee . The Journal of Arthroplasty . 2015 ; 30 ( 12 ): 2149 – 2153 . Crossref PubMed Google Scholar
17. Demange MK , Von Keudell A , Probst C , Yoshioka H , Gomoll AH . Patient-specific implants for lateral unicompartmental knee arthroplasty . Int Orthop . 2015 ; 39 ( 8 ): 1519 – 1526 . Crossref PubMed Google Scholar
18. Steklov N , Slamin J , Srivastav S , D'Lima D . Unicompartmental knee resurfacing: enlarged tibio-femoral contact area and reduced contact stress using novel patient-derived geometries . Open Biomed Eng J . 2010 ; 4 : 485 – 492 . Crossref PubMed Google Scholar
19. Koh YG , Lee JA , Lee HY , et al. Reduction in tibiofemoral conformity in lateral unicompartmental knee arthroplasty is more representative of normal knee kinematics . Bone Joint Res . 2019 ; 8 ( 12 ): 593 – 600 . Crossref PubMed Google Scholar
20. Kang KT , Koh YG , Son J , et al. Biomechanical influence of deficient posterolateral corner structures on knee joint kinematics: A computational study . J Orthop Res . 2018 : 2202 – 2209 . Crossref PubMed Google Scholar
21. Kang KT , Koh YG , Park KM , et al. The anterolateral ligament is a secondary stabilizer in the knee joint: A validated computational model of the biomechanical effects of a deficient anterior cruciate ligament and anterolateral ligament on knee joint kinematics . Bone Joint Res . 2019 ; 8 ( 11 ): 509 – 517 . Crossref PubMed Google Scholar
22. Kang KT , Koh YG , Nam JH , et al. Biomechanical evaluation of the influence of posterolateral corner structures on cruciate ligaments forces during simulated gait and squatting . PLoS One . 2019 ; 14 ( 4 ): e0214496 . Crossref PubMed Google Scholar
23. Kang KT , Son J , Suh DS , et al. Patient-specific medial unicompartmental knee arthroplasty has a greater protective effect on articular cartilage in the lateral compartment: A Finite Element Analysis . Bone Joint Res . 2018 ; 7 ( 1 ): 20 – 27 . Crossref PubMed Google Scholar
24. Kang KT , Koh YG , Son J , et al. Finite Element Analysis of the Biomechanical Effects of 3 Posterolateral Corner Reconstruction Techniques for the Knee Joint . J Arthroscopy . 2017 ; 33 ( 8 ): 1537 – 1550 . Crossref PubMed Google Scholar
25. Blankevoort L , Huiskes R . Validation of a three-dimensional model of the knee . J Biomech . 1996 ; 29 ( 7 ): 955 – 961 . Crossref PubMed Google Scholar
26. Mesfar W , Shirazi-Adl A . Biomechanics of the knee joint in flexion under various quadriceps forces . The Knee . 2005 ; 12 ( 6 ): 424 – 434 . Crossref PubMed Google Scholar
27. Godest AC , Beaugonin M , Haug E , Taylor M , Gregson PJ . Simulation of a knee joint replacement during a gait cycle using explicit finite element analysis . J Biomech . 2002 ; 35 ( 2 ): 267 – 275 . Crossref PubMed Google Scholar
28. Inoue S , Akagi M , Asada S , et al. The Valgus Inclination of the Tibial Component Increases the Risk of Medial Tibial Condylar Fractures in Unicompartmental Knee Arthroplasty . J Arthroplasty . 2016 ; 31 ( 9 ): 2025 – 2030 . Crossref PubMed Google Scholar
29. Koh YG , Lee JA , Lee HY , Kim HJ , Kang KT . Computational wear prediction of insert conformity and material on mobile-bearing unicompartmental knee arthroplasty . Bone Joint Res . 2019 ; 8 ( 11 ): 563 – 569 . Crossref PubMed Google Scholar
30. Pena E , Calvo B , Martinez MA , Palanca D , Doblare M . Why lateral meniscectomy is more dangerous than medial meniscectomy. A finite element study . J Orthop Res . 2006 ; 24 ( 5 ): 1001 – 1010 . Crossref PubMed Google Scholar
31. Kang KT , Koh YG , Son J , Kwon OR , Park KK . Flexed femoral component improves kinematics and biomechanical effect in posterior stabilized total knee arthroplasty . Knee Surg Sports Traumatol Arthrosc . 2018 ; 27 ( 4 ): 1174 – 1181 . Crossref PubMed Google Scholar
32. Kutzner I , Heinlein B , Graichen F , et al. Loading of the knee joint during activities of daily living measured in vivo in five subjects . J Biomech . 2010 ; 43 ( 11 ): 2164 – 2173 . Crossref PubMed Google Scholar
33. Grood ES , Suntay WJ . A joint coordinate system for the clinical description of three-dimensional motions: application to the knee . J Biomech Eng . 1983 ; 105 ( 2 ): 136 – 144 . Crossref PubMed Google Scholar
34. Insall JN , Dorr LD , Scott RD , Scott WN . Rationale of the Knee Society clinical rating system . Clin Orthop Relat Res . 1989 ( 248 ): 13 – 14 . PubMed Google Scholar
35. Nakagawa S , Kadoya Y , Todo S , et al. Tibiofemoral movement 3: full flexion in the living knee studied by MRI . J Bone Joint Surg Br . 2000 ; 82-B ( 8 ): 1199 – 1200 . Crossref PubMed Google Scholar
36. Johal P , Williams A , Wragg P , Hunt D , Gedroyc W . Tibio-femoral movement in the living knee. A study of weight bearing and non-weight bearing knee kinematics using 'interventional' MRI . J Biomech . 2005 ; 38 ( 2 ): 269 – 276 . Crossref PubMed Google Scholar
37. Komistek RD , Dennis DA , Mahfouz M . In vivo fluoroscopic analysis of the normal human knee . Clin Orthop Relat Res . 2003 ; 410 : 69 – 81 . Crossref PubMed Google Scholar
38. Li J-S , Hosseini A , Cancre L , et al. Kinematic characteristics of the tibiofemoral joint during a step-up activity . Gait Posture . 2013 ; 38 ( 4 ): 712 – 716 . Crossref PubMed Google Scholar
39. Moro-oka TA , Hamai S , Miura H , et al. Dynamic activity dependence of in vivo normal knee kinematics . J Orthop Res . 2008 ; 26 ( 4 ): 428 – 434 . Crossref PubMed Google Scholar
40. Koh YG , Son J , Kwon OR , Kwon SK , Kang KT . Patient-specific design for articular surface conformity to preserve normal knee mechanics in posterior stabilized total knee arthroplasty . Biomed Mater Eng . 2018 ; 29 ( 4 ): 401 – 414 . Crossref PubMed Google Scholar
41. Koh YG , Son J , Kwon OR , Kwon SK , Kang KT . Tibiofemoral conformity variation offers changed kinematics and wear performance of customized posterior-stabilized total knee arthroplasty . Knee Surg Sports Traumatol Arthrosc . 2019 ; 27 ( 4 ): 1213 – 1223 . Crossref PubMed Google Scholar
42. Altuntas AO , Alsop H , Cobb JP . Early results of a domed tibia, mobile bearing lateral unicompartmental knee arthroplasty from an independent centre . Knee . 2013 ; 20 ( 6 ): 466 – 470 . Crossref PubMed Google Scholar
43. Hallen LG , Lindahl O . The "screw-home" movement in the knee-joint . Acta Orthop Scand . 1966 ; 37 ( 1 ): 97 – 106 . Google Scholar
44. Wilson DR , Feikes JD , Zavatsky AB , O'Connor JJ . The components of passive knee movement are coupled to flexion angle . J Biomech . 2000 ; 33 ( 4 ): 465 – 473 . Crossref PubMed Google Scholar
45. Patil S , Colwell CW , Ezzet KA , D'Lima DD . Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am . 2005 ; 87-A ( 2 ): 332 – 338 . Crossref PubMed Google Scholar
46. Rajendran K . Mechanism of locking at the knee joint . J Anat . 1985 ; 143 : 143189 – 143194 . PubMed Google Scholar
47. Wada K , Hamada D , Takasago T , et al. Native rotational knee kinematics is restored after lateral UKA but not after medial UKA . Knee Surg Sports Traumatol Arthrosc . 2018 ; 26 ( 11 ): 3438 – 3443 . Google Scholar
Author contributions
Y-G. Koh and J-A. Lee are joint first authors.
Y-G. Koh: Drafted the manuscript.
J-A. Lee: Developed the 3D model.
H-S. Chung: Evaluated the data.
H-J. Kim: Interpreted the data.
K-T. Kang: Supervised the study.
Y-G. Koh and J-A. Lee contributed equally to this work.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Acknowledgements
No external source of funding was received for the study.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial No Derivatives (CC BY-NC-ND 4.0) licence, which permits the copying and redistribution of the work only, and provided the original author and source are credited. See https://creativecommons.org/licenses/by-nc-nd/4.0/.
