




Abstract
Aims
This study aimed to investigate the relationship between changes in patellar height and clinical outcomes at a mean follow-up of 7.7 years (5 to 10) after fixed-bearing posterior-stabilized total knee arthroplasty (PS-TKA).
Methods
We retrospectively evaluated knee radiographs of 165 knees, which underwent fixed-bearing PS-TKA with patella resurfacing. The incidence of patella baja and changes in patellar height over a minimum of five years of follow-up were determined using Insall-Salvati ratio (ISR) measurement. We examined whether patella baja (ISR < 0.8) at final follow-up affected clinical outcomes, knee joint range of motion (ROM), and Knee Society Score (KSS). We also assessed inter- and intrarater reliability of ISR measurements and focused on the relationship between patellar height reduction beyond measurement error and clinical outcomes.
Results
The ISR gradually decreased over five years after TKA, and finally 33 patients (20.0%) had patella baja. Patella baja at the final follow-up was not related to passive knee ROM or KSS. Interestingly, when we divided into two groups - patella baja and patella normal-alta (ISR ≥ 0.8) - the patella baja group already had a lower patellar height before surgery, compared with the patella normal-alta group. The ISR measurement error in this study was 0.17. Both passive knee flexion and KSS were significantly decreased in the group with a decrease in ISR of ≥ 0.17 at final follow-up.
Conclusion
Patellar height gradually decreased over five years of follow-up after TKA. The reduction in patellar height beyond measurement error following TKA was associated with lower clinical outcomes.
Cite this article: Bone Jt Open 2021;2(12):1075–1081.
Take home message
In this study, patella baja (Insall-Salvati ratio < 0.8) progressed by five years after fixed-bearing posterior-stabilized total knee arrthroplasty (TKA), and was not associated with clinical outcomes or knee range of motion.
On the other hand, a significant decrease in patellar height beyond the minimal detectable change was associated with passive knee flexion and decreased Knee Society Score after TKA. Thus, cases with a significant decrease in patellar height might have a worse postoperative outcome.
Introduction
Patella baja has been associated with several etiologies, including fractures around the knee,1 anterior cruciate ligament reconstruction,2 and high tibial osteotomy (HTO).3,4 Several studies have shown the adverse effects of inferior patellar position after total knee arthroplasty (TKA).5-10 These include altered joint mechanics, decreased lever arm and extensor lag, reduction in range of motion (ROM), anterior knee pain, a possible cause of increased tibial and patellar polyethylene wear, and reduced long-term implant survival. This potentially disabling syndrome must be recognized early in its course so that prompt treatment can be initiated. Previous studies have shown that the patellar tendon continues to shorten from six months to one year and then plateaus.11-15 Little information is available about long-term follow-up beyond five years, the pattern of changes in patellar height over time, or whether changes in patellar height are predictable. The purpose of the present study was to determine the incidence of patella baja over five years in fixed-bearing posterior-stabilized (PS)-TKA using the Insall-Salvati ratio (ISR)16 and the association between postoperative patella baja and knee ROM and the Knee Society Score (KSS).17 In addition, we investigated the measurement error of ISR and the impact of postoperative decrease in patellar height on clinical outcomes.
Methods
Patient selection
Between January 2010 and January 2012, 216 consecutive primary cemented TKA cases (NexGen LPS flex system; Zimmer Biomet, USA) with fixed-bearing and posterior stabilization in all knees were performed in Ogori Daiichi General Hospital, Japan, by two senior surgeons (HF, YA). High-flex femur and keel tibial baseplate were used in all cases. The surgical approach was a standard medial parapatellar approach with patella eversion using a modified gap balancing technique. The infrapatellar fat pad was partially (approximately 70%) resected, and the patella was resurfaced in all patients. Lateral retinacular release was not performed in any patients. Passive and active knee ROM exercises were initiated the day after surgery. In the present study, we retrospectively included 165 knees (136 patients; 20 males and 116 females) with mean age was 75.4 years (56 to 86), which were available for review with a mean follow-up of 7.7 years (5 to 10). For the diagnosis that underwent TKA, there were 157 cases of degenerative knee osteoarthritis and eight cases of spontaneous osteonecrosis of the knee. Right side was 79 knees, and left side was 86 knees. Overall, 51 knees were excluded because of incomplete data in 11 cases, lost to follow-up in 21 cases, prior arthroscopic debridement in six cases, post-trauma in four cases, periprosthetic fracture in three cases, ipsilateral proximal femur fracture in two cases, ipsilateral total hip arthroplasty in two cases, prior HTO in one case, and infection in one case.
Data collection
A lateral radiograph of the knee was taken at approximately 30° of flexion. We assessed the pre- and postoperative ISR and its changes in all patients. In addition to the radiological evaluation, clinical data, including postoperative knee ROM and KSS, were obtained. Our institutional review board approved the study and waived the requirement for informed consent because it was a retrospective study using existing medical records and posed minimal risk to patients (No. 15-08).
Statistical analysis
To evaluate the patellar height, the length of the patellar tendon and the longest portion of the patella were measured using computer software (FS-V673; FUJIFILM, Japan).
The ISR was calculated by dividing the length of the patellar tendon by the length of the longest portion of the patella measured from lateral radiographs with the knee in flexion. Patella baja was defined as having an ISR of < 0.8, based on the original paper described by Insall et al.16 We investigated whether the conventional criteria of patella baja (ISR < 0.8) at final follow-up affected the clinical outcomes.
In addition, to examine the effect of reduction in patellar height itself on clinical outcomes, rather than the traditional criterion of patella baja (ISR < 0.8), we focused on the measurement error of ISR and investigated the relationship between patellar tendon shortening itself beyond the measurement error and clinical outcomes. Inter-rater and intra-rater reliability of the measurements were also assessed by two senior orthopaedic surgeons (HF, KY). In all, 20 random samples of lateral knee radiographs were selected from the data of 165 knees. Each knee was examined twice with an interval of at least one week. Each observer measured the ISR. Inter- and intrarater reliability was assessed by intraclass correlation coefficients (ICCs) and Bland-Altman analysis.18 The interpretation of the ICC value was based on the criteria proposed by Landis et al.19 The reliability of an ICC over 0.81 is considered to be almost perfect, and between 0.61 and 0.8 to be substantial. A value of an ICC less than 0.60 was not accepted for the test and retest methods. Absolute reliability was assessed by the standard error of measurement (SEM) and minimal detectable change at 95% confidence level (MDC95). The ICC, MDC, and Bland-Altman analyses of ISR measurements are shown in Table I and Table II. The ICC (γ) for inter-and intrarater reliability was greater than 0.9 (Table III); Bland-Altman analysis also showed excellent intra- and inter-rater reproducibility; MDC 95 was 0.169 for rater 1, 0.127 for rater 2, and 0.134 for inter-rater (Table IV). These data suggest that significant changes occurred when the ISR changed above 0.17. Data were represented as mean (standard deviation (SD)). Differences were analyzed using Student's t-test or paired t-test; p-values < 0.05 were considered statistically significant.
Table I.
Incidence of patella baja at each follow-up.
| Variable | Pre-surgery | Surgery | 2 months | 6 months | 1 year | 2 years | 5 years | Final (7.7 years) |
|---|---|---|---|---|---|---|---|---|
| Cases, n (%) | 4 (2.4) | 3 (1.8) | 2 (1.2) | 4 (2.4) | 12 (7.3) | 23 (13.9) | 33 (20.0) | 33 (20.0) |
Table II.
Association between patella baja and clinical outcomes at the final follow-up.
| Variable | ISR < 0.8 (n = 33), mean (SD) | ISR ≥ 0.8 (n = 132), mean (SD) | p-value* |
|---|---|---|---|
| Age, yrs | 74.9 (6.2) | 75.5 (5.5) | 0.628 |
| BMI, kg/m2 | 26.7 (6.2) | 25.5 (3.2) | 0.128 |
| Knee extension, ° | -2.3 (5.2) | -3.1 (5.5) | 0.424 |
| Knee flexion,° | 122.4 (13.1) | 125.9 (12.6) | 0.155 |
| KSS | 81.8 (11.4) | 84.8 (8.7) | 0.102 |
-
*
Student's t-test.
-
ISR, Insall-Salvati ratio; KSS, Knee Society Score; SD, standard deviation.
Table III.
Intraclass correlation coefficient (ICC) for Insall-Salvati ratio.
| Variable | ICC estimate (95% CI) |
|---|---|
| Inter-rater 1 | 0.92 (0.817 to 0.967) |
| Inter-rater 2 | 0.992 (0.981 to 0.997) |
| Inter-rater | 0.925 (0.720 to 0.974) |
-
CI, confidence interval.
Table IV.
Bland-Altman analysis for Insall-Salvati ratio (ISR).
| ISR | First, mean (SD) | Second, mean (SD) | Bias | SEM | 95% CI | MDC95 |
|---|---|---|---|---|---|---|
| Intrarater 1 | 1.016 (0.169) | 0.991 (0.147) | 0.024 | 0.061 | -0.052 to 0.003 | 0.169 |
| Intrarater 2 | 1.026 (0.162) | 1.016 (0.149) | 0.011 | 0.046 | -0.032 to 0.010 | 0.127 |
| Rater 1 | Rater 2 | |||||
| Inter-rater (first) | 1.016 (0.169) | 1.026 (0.162) | 0.035 | 0.048 | -0.057 to 0.013 | 0.134 |
-
CI, confidence interval; MDC95, minimal detectable change at 95% confidence level; SD, standard deviation
Results
We selected serial radiographs of the affected knees taken on pre-surgery, immediately after surgery, at two months, six months, one year, two years, five years, and at last follow-up after surgery (mean 7.7 years; 5 to 10). Using ISR, the mean patellar height before TKA was 1.03 (0.64 to 1.46), which significantly decreased at the one-year follow-up (p = 0.003, paired t-test), and further continued to decrease to 0.94 (0.45 to 1.40) at the final follow-up (mean 7.7 years (5 to 10)) (Figure 1). The incidence of patella baja in this series (ISR < 0.8) was 2.4% (n = 4) before surgery, 1.8% (n = 3) immediately after surgery, 1.2% (n = 2) at two months, 2.4% (n = 4) at six months, 7.3% (n = 12) at one year, 13.9% (n = 23) at two years, 20.0% (n = 33) at five years, and 20.0% (n = 33) at final follow-up (Table I).
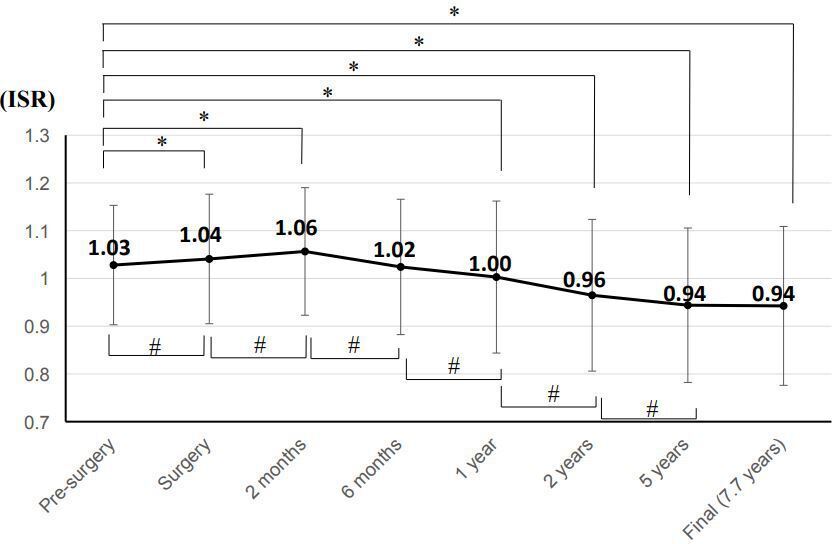
Fig. 1
Mean Insall-Salvati ratio of all patients at each follow-up. Data are shown as mean (standard deviation). *p < 0.05.
We divided the knees into two groups: the patella baja group (ISR < 0.8 at the final follow-up; n = 33), and the patella normal-alta group (ISR ≥ 0.8 at the final follow-up; n = 132). In the patella baja group, there was no difference in knee ROM (Table II). For the clinical outcomes, the patella baja group had lower scores than the patella normal-alta group, but there was no significant difference between the two groups. The mean ISR of these two groups at each follow-up was then plotted on a graph (as shown in Figure 2). The results showed that the mean ISR in the patella baja group decreased significantly from six months after surgery to the final follow-up. In the patella baja group, the ISR was already lower than that of the normal-alta group before surgery (p <0.001, Student's t-test; Figure 2).
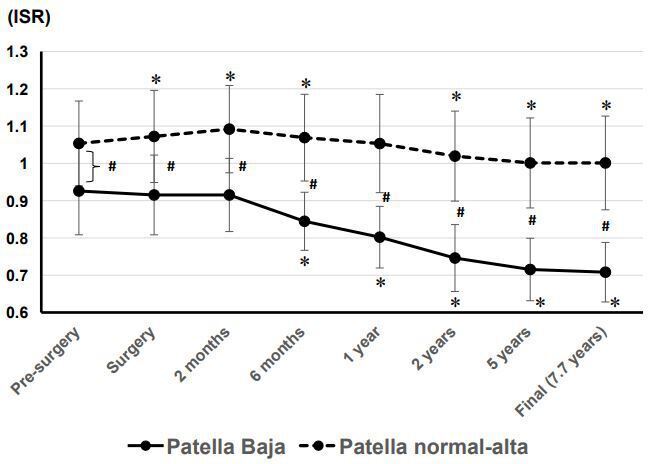
Fig. 2
Mean Insall-Salvati ratio of patella baja group and normal-alta group at pre-surgery, zero, two, six, 12, 24, and 60 months and final follow-up after surgery. Data are shown as mean (standard deviation). *p < 0.05 compared between pre-surgery and each follow-up time point. p < 0.05 compared between two groups.
Next, we divided the knees into two groups: group A (patellar height descend beyond MDC 0.17; n = 33) and group B (patellar height did not descend above MDC 0.17; n = 132) (Figure 3). Group A had a statistically significant decrease in patellar height at two months after surgery, and it was gradually decreased throughout the observation period. However, patellar height in group B did not decrease until two years after TKA. Clinically, group A had a statistically significant decrease in passive knee flexion (p = 0.008, Student's t-test), Table V), but knee extension did not reduce. In addition, group A had significant less scores compared to group B (p = 0.012, Student's t-test) (Table V). Thus, these data indicate that significant patellar height reduction is an independent factor in reduced knee flexion and KSS after fixed-bearing PS-TKA.
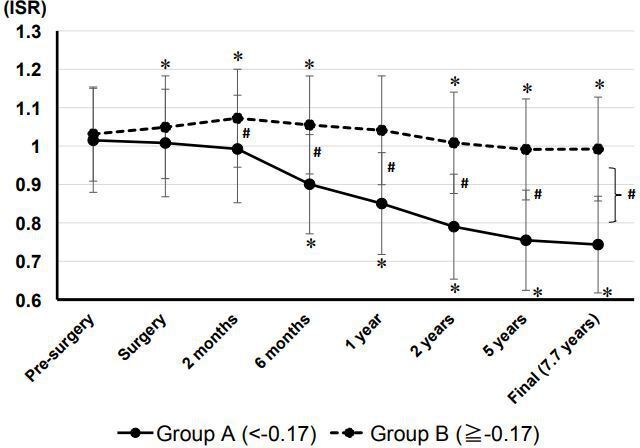
Fig. 3
Mean Insall-Salvati ratio of group A (change of patellar height < -0.17) and group B (change of patellar height ≧ -0.17) at pre-surgery, zero, two, six, 12, 24, and 60 months and the final follow-up after surgery. Data are shown as mean (standard deviation). *p < 0.05 compared between pre-surgery and each follow-up time point. p < 0.05 compared between two groups.
Table V.
Association between significant shortening of patellar height and clinical outcomes at final follow-up.
| Variable | Group A (< −0.17) (n = 33) | Group B (≥ −0.17) (n = 132) | p-value* |
|---|---|---|---|
| Age, yrs | 73.8 (96.3) | 75.8 (5.5) | 0.079 |
| BMI, kg/m2 | 27.0 (6.3) | 25.4 (3.1) | 0.048 |
| Knee extension, ° | -1.9 (4.9) | -3.2 (5.6) | 0.219 |
| Knee flexion, ° | 120.0 (13.3) | 126.6 (12.3) | 0.008 |
| KSS | 80.5 (11.8) | 85.1 (8.4) | 0.012 |
-
*
Student's t-test.
-
KSS, Knee Society Score; SD, standard deviation.
Discussion
In the present study, the incidence of patella baja after fixed-bearing PS-TKA was 20.0% with a mean follow-up of 7.7 years. Similarly, Meneghini et al20 reported patella baja in 16.4% (173/1,055 knees, including 956 posterior cruciate ligament-retaining TKAs and 109 posterior cruciate-substituting TKAs) with a mean follow-up of 5.1 years using ISR < 0.8. They also described that patella baja appeared to occur after TKA with or without posterior cruciate ligament retaining. Incidence of decreased patellar height after TKA ranged from 0.7% to 65% in previous reports, although the measurement method and criteria vary.11,13,14 Most of this reduction was observed in six months postoperatively, after which only mild shortening was noted.11-15 In our study, patients continued to develop patella baja until five years later. Recently, Davies et al21 also reported that the ISR of TKA patients continued to shorten from year one to year five.
The aetiology of patellar height reduction after TKA is still unclear, and probably multifactorial; surgical procedures such as lateral retinacular release, infrapatellar fat pad resection, and patellar eversion have been suggested as possible causes of patella tendon shortening following TKA. Lateral release and fat pad excision could lead to ischaemia of the patella tendon, resulting in shortening of the patellar tendon.22 Weale et al23 found a highly significant reduction in patellar tendon length after eight months in 34% of their TKAs requiring lateral release, compared with 24% in those that did not need a lateral release. Lemon et al13 compared the difference in the change of patellar tendon length between completely fat pad preservation and complete excision. After three years, there was a significant patellar tendon shortening of 4.2% in the excision group and no significant change in the preservation group. Regarding patellar eversion, Floren et al11 reported that the incidence of patella baja was reduced from 37% to 12% when the patella was only displaced but not everted. In contrast, Sharma et al12 described that postoperative patella baja was only 0.7% (one of 135 knees) after the patellar eversion procedure. In our series, approximately 70% fat pad resection and patellar eversion were performed in all cases, although the lateral release was not performed, and we speculated that these techniques influenced the occurrence of patella baja, and patellar resurfacing during the procedure in all cases, without lateral release. Interestingly, our results indicated that patients with postoperative patella baja already had a preoperative lower patellar height. These data suggest that preoperative characteristics of the patellar tendon also influence the development of patella baja in addition to the intraoperative peripatellar manipulation.
In this study, we examined the impact on clinical outcomes from two perspectives: the conventional definition of patella baja (ISR < 0.8) and the reduction in ISR beyond the measurement error (0.17). This study demonstrated that a decrease in patellar height above the measurement error, but not patella baja (ISR < 0.8), was significantly associated with reduced knee ROM and KSS. In the past studies, changes in patellar tendon length after TKA was associated with decreased postoperative knee ROM,23 anterior knee pain, anterior polyethylene impingement and wear, and decreased outcomes,7,10,14,23-25 but recent studies have found no correlation between ISR and knee ROM and clinical scores, such as the Oxford Knee Score, KSS, and Hospital for Special Surgery Score.12,15,20,21,23,26 This difference in the correlation between the lower patellar height and the clinical outcomes among the papers may be due in part to the different evaluation criteria. In fact, we found no significant difference in knee ROM and clinical outcome when the general patella baja (ISR < 0.8) was used as the criterion, but we did find a difference in clinical outcomes when another criterion (patellar height descend beyond MDC) was used.
Limitations
There are several limitations in the present study. First, this was a retrospective analysis, and the exact amount of fat pad excision and rehabilitation intervention was unclear. Second, we used the ISR to analyze the patellar height after TKA. Measuring ISR has some drawbacks; for example, bony landmarks are not always easy to identify, the size of the patella can vary, and pathological bony overgrowth can distort the native anatomy.27-29 However, the modern digital radiographs have such good soft-tissue definition that the patellar tendon itself is usually visible, making accurate identification of the tibial tubercle obsolete.30 In addition, a cadaveric study by Schlenzka et al31 demonstrated that the absolute values of anatomical measurements and the resulting ISR correlated well with the ratios measured on lateral radiographs. Third, ROM was measured by one senior orthopaedic surgeon (HF) using a goniometer with a precision of 5°. The measurement error was not evaluated for knee ROM measurements. Finally, our study showed that a significant decrease in patellar height after TKA reduced KSS, but the difference was only 4.6 points. Lizaur-Utrilla et al32 reported that the minimal clinical important difference for the KSS after TKA was at least nine points. Thus, the impact on knee function for the reduced patellar height following TKA seems to be small.
In conclusion, the present study indicated that patella baja (ISR < 0.8) progressed up to five years postoperatively and was not related to clinical outcome, but the decrease in patellar height beyond the measurement error between the surgery and final follow-up was associated with a decrease in passive knee flexion and KSS after fixed-bearing PS-TKA. The reduction in patellar height after TKA may not occur in all patients who underwent partial fat pad resection and patella eversion, but is more likely to occur in some patients, especially those with preoperative lower patellar height. Thus, further studies are needed to prevent shortening of patellar height in patients with low preoperative patellar height through therapeutic interventions, such as fat pad preservation and long-term rehabilitation. The reduction of patellar height and long-term implant survival should also be investigated.
References
1. Mariani PP , Del Signore S , Perugia L . Early development of patella infera after knee fractures . Knee Surg Sports Traumatol Arthrosc . 1994 ; 2 ( 3 ): 166 – 169 . Crossref PubMed Google Scholar
2. Dandy DJ , Desai SS . Patellar tendon length after anterior cruciate ligament reconstruction . J Bone Joint Surg Br . 1994 ; 76-B ( 2 ): 198 – 199 . Crossref PubMed Google Scholar
3. Okamoto R , Koshino T , Morii T . Shortening of patellar ligament and patella baja with improvement of quadriceps muscle strength after high tibial osteotomy . Bull Hosp Jt Dis . 1993 ; 53 ( 3 ): 21 – 24 . PubMed Google Scholar
4. Scuderi GR , Windsor RE , Insall JN . Observations on patellar height after proximal tibial osteotomy . J Bone Joint Surg Am . 1989 ; 71-A ( 2 ): 245 – 248 . PubMed Google Scholar
5. Ahmad CS . Effects of patellar tendon adhesion to the anterior tibia on knee mechanics . Am J Sports Med . 1998 ; 26 ( 5 ): 715 – 724 . Crossref PubMed Google Scholar
6. Browne C , Hermida JC , Bergula A , Colwell CW, Jr. , D’Lima DD . Patellofemoral forces after total knee arthroplasty: effect of extensor moment arm . Knee . 2005 ; 12 ( 2 ): 81 – 88 . Crossref PubMed Google Scholar
7. Figgie HE , Goldberg VM , Heiple KG , Moller HS , Gordon NH . The influence of tibial-patellofemoral location on function of the knee in patients with the posterior stabilized condylar knee prosthesis . J Bone Joint Surg Am . 1986 ; 68-A ( 7 ): 1035 – 1040 . PubMed Google Scholar
8. Laskin RS , Beksac B . Stiffness after total knee arthroplasty . J Arthroplasty . 2004 ; 19 ( 4 Suppl 1 ): 41 – 46 . Crossref PubMed Google Scholar
9. Lee GC , Cushner FD , Scuderi GR , Insall JN . Optimizing patellofemoral tracking during total knee arthroplasty . J Knee Surg . 2004 ; 17 ( 3 ): 144 – 149 . Crossref PubMed Google Scholar
10. Yoshii I , Whiteside LA , White SE , Milliano MT . Influence of prosthetic joint line position on knee kinematics and patellar position . J Arthroplasty . 1991 ; 6 ( 2 ): 169 – 177 . Crossref PubMed Google Scholar
11. Floren M , Davis J , Peterson MG , Laskin RS . A mini-midvastus capsular approach with patellar displacement decreases the prevalence of patella baja . J Arthroplasty . 2007 ; 22 ( 6 Suppl 2 ): 51 – 57 . Crossref PubMed Google Scholar
12. Sharma V , Tsailas PG , Maheshwari AV , Ranawat AS , Ranawat CS . Does patellar eversion in total knee arthroplasty cause patella baja . Clin Orthop Relat Res . 2008 ; 466 ( 11 ): 2763 – 2768 . Crossref PubMed Google Scholar
13. Lemon M , Packham I , Narang K , Craig DM . Patellar tendon length after knee arthroplasty with and without preservation of the infrapatellar fat pad . J Arthroplasty . 2007 ; 22 ( 4 ): 574 – 580 . Crossref PubMed Google Scholar
14. Koshino T , Ejima M , Okamoto R , Morii T . Gradual low riding of the patella during the postoperative course after total knee arthroplasty in osteoarthritis and rheumatoid arthritis . J Arthroplasty . 1990 ; 5 ( 4 ): 323 – 327 . Google Scholar
15. Ishii Y , Noguchi H , Sato J , Ishii H , Ezawa N , Toyabe SI . Insall-salvati ratio stabilizes one year after mobile-bearing total knee arthroplasty and does not correlate with mid-to-long-term clinical outcomes . Knee Surg Sports Traumatol Arthrosc . 2019 ; 27 ( 5 ): 1604 – 1610 . Google Scholar
16. Insall J , Salvati E . Patella position in the normal knee joint . Radiology . 1971 ; 101 ( 1 ): 101 – 104 . Crossref PubMed Google Scholar
17. Insall JN , Dorr LD , Scott RD , Scott WN . Rationale of the knee Society clinical rating system . Clin Orthop Relat Res . 1989 ; 248 : 13 – 14 . PubMed Google Scholar
18. Bland JM , Altman DG . Statistical methods for assessing agreement between two methods of clinical measurement . Lancet . 1986 ; 1 : 307 – 310 . PubMed Google Scholar
19. Landis JR , Koch GG . The measurement of observer agreement for categorical data . Biometrics . 1977 ; 33 ( 1 ): 159 – 174 . PubMed Google Scholar
20. Meneghini RM , Ritter MA , Pierson JL , Meding JB , Berend ME , Faris PM . The effect of the Insall-Salvati ratio on outcome after total knee arthroplasty . J Arthroplasty . 2006 ; 21 ( 6 Suppl 2 ): 116 – 120 . Crossref PubMed Google Scholar
21. Davies GS , van Duren B , Shorthose M , et al. Changes in patella tendon length over 5 years after different types of knee arthroplasty . Knee Surg Sports Traumatol Arthrosc . 2016 ; 24 ( 9 ): 3029 – 3035 . Google Scholar
22. Kayler DE , Lyttle D . Surgical interruption of patellar blood supply by total knee arthroplasty . Clin Orthop Relat Res . 1988 ; 229 : 207 . PubMed Google Scholar
23. Weale AE , Murray DW , Newman JH , Ackroyd CE . The length of the patellar tendon after unicompartmental and total knee replacement . J Bone Joint Surg Br . 1999 ; 81-B ( 5 ): 790 – 795 . Crossref PubMed Google Scholar
24. Cameron HU , Jung YB . Patella Baja complicating total knee arthroplasty. A report of two cases . J Arthroplasty . 1988 ; 3 ( 2 ): 177 – 180 . PubMed Google Scholar
25. Grelsamer RP . Patella baja after total knee arthroplasty: is it really patella baja . J Arthroplasty . 2002 ; 17 ( 1 ): 66 – 69 . Crossref PubMed Google Scholar
26. Reid MJ , Booth G , Khan RJ , Janes G . Patellar eversion during total knee replacement: a prospective, randomized trial . J Bone Joint Surg Am . 2014 ; 96-A ( 3 ): 207 – 213 . Crossref PubMed Google Scholar
27. Burgess RC . A new method of determining patellar position . J Sports Med Phys Fitness . 1989 ; 29 ( 4 ): 389 – 9 . PubMed Google Scholar
28. Grelsamer RP , Proctor CS , Bazos AN . Evaluation of patellar shape in the sagittal plane. A clinical analysis . Am J Sports Med . 1994 ; 22 ( 1 ): 61 – 66 . Crossref PubMed Google Scholar
29. Seil R , Müller B , Georg T , Kohn D , Rupp S . Reliability and interobserver variability in radiological patellar height ratios . Knee Surg Sports Traumatol Arthrosc . 2000 ; 8 ( 4 ): 231 – 236 . Crossref PubMed Google Scholar
30. Phillips CL , Silver DA , Schranz PJ , Mandalia V . The measurement of patellar height: a review of the methods of imaging . J Bone Joint Surg Br . 2010 ; 92-B ( 8 ): 1045 – 1053 . Crossref PubMed Google Scholar
31. Schlenzka D , Schwesinger G . The height of the patella: an anatomical study . Eur J Radiol . 1990 ; 11 ( 1 ): 19 – 21 . Crossref PubMed Google Scholar
32. Lizaur-Utrilla A , Gonzalez-Parreño S , Martinez-Mendez D , Miralles-Muñoz FA , Lopez-Prats FA . Minimal clinically important differences and substantial clinical benefits for knee society scores . Knee Surg Sports Traumatol Arthrosc . 2020 ; 28 ( 5 ): 1473 – 1478 . Crossref PubMed Google Scholar
Author contributions
A. Suthar: Investigation, Formal analysis, Writing – original draft.
K. Yukata: Conceptualization, Investigation, Formal analysis, Writing – review & editing.
Y. Azuma: Writing – review & editing.
Y. Suetomi: Writing – review & editing.
K. Yamazaki: Formal analysis, Writing – review & editing.
K. Seki: Writing – review & editing.
T. Sakai: Writing – review & editing.
H. Fujii: Conceptualization, Writing – review & editing.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
ICMJE COI statement
All authors confirm that they have no conflicts of interest.
Ethical review statement
This study was reviewed and approved by our Insitutional Review Board (#15-08).
