




Abstract
Aims
The worldwide COVID-19 pandemic is directly impacting the field of orthopaedic surgery and traumatology with postponed operations, changed status of planned elective surgeries and acute emergencies in patients with unknown infection status. To this point, Germany's COVID-19 infection numbers and death rate have been lower than those of many other nations.
Methods
This article summarizes the current regimen used in the field of orthopaedics in Germany during the COVID-19 pandemic. Internal university clinic guidelines, latest research results, expert consensus, and clinical experiences were combined in this article guideline.
Results
Every patient, with and without symptoms, should be screened for COVID-19 before hospital admission. Patients should be assigned to three groups (infection status unknown, confirmed, or negative). Patients with unknown infection status should be considered as infectious. Dependent of the infection status and acuity of the symptoms, patients are assigned to a COVID-19-free or affected zone of the hospital. Isolation, hand hygiene, and personal protective equipment is essential. Hospital personnel directly involved in the care of COVID-19 patients should be tested on a weekly basis independently of the presence of clinical symptoms, staff in the COVID-19-free zone on a biweekly basis. Class 1a operation rooms with laminar air flow and negative pressure are preferred for surgery in COVID-19 patients. Electrocautery should only be utilized with a smoke suction system. In cases of unavoidable elective surgery, a self-imposed quarantine of 14 days is recommended prior to hospital admission.
Conclusion
During the current COVID-19 pandemic, orthopaedic patients admitted to the hospital should be treated based on an interdisciplinary algorithm, strictly separating infectious and non-infectious cases.
Cite this article: Bone Joint Open 2020;1-6:309–315.
Introduction
The new coronavirus SARS-CoV-2 (COVID-19) has spread with alarming speed and frightening magnitude to turn it into a global pandemic with significant impact on the care of orthopaedic and traumatological patients. With globally increasing numbers of infected patients and the resulting restrictions on the elective surgical care of musculoskeletal patients, orthopaedic surgeons are faced with challenges in providing continuity of care to musculoskeletal patients, while ensuring the safety of patients and hospital personnel.
The COVID-19 virus spreads via aerosols of the respiratory tract and nasal cavities, with small particles remaining airborne for multiple hours, or via direct contact with infected patients or indirectly through contaminated surfaces.1-4 Hospital staff are at increased risk for COVID-19 infection and can unknowingly spread it during all phases of patient care including hospital admission, outpatient clinics, inpatient care, and surgery.5 Epidemiological data from China confirm an extremely high infection risk for hospital staff with mortality rates of up to 3%.6-8 As of 17 April 2020, the Italian National Federation for the Orders of Doctors and Dentists (FNOMCeO) reported over 131 physician deaths due to COVID-19. It is important to note that it is not only COVID-19 patients that pose a high infection risk; it can also originate from asymptomatic COVID-19-positive carriers. Current investigations confirm that asymptomatic carriers have similar viral loads in their upper respiratory tract compared to symptomatic patients and can therefore spread COVID-19 with similar infectiousness.1 Therefore, a strict hygiene protocol and a restructuring of hospital procedure is necessary to safely treat patients during the COVID-19 pandemic.
Methods
This article presents a combined guideline out of two German university clinic systems used during the COVID-19 pandemic in the field of orthopaedic surgery and traumatology. The first clinic is the Centre for Musculoskeletal Surgery at the Charité University Medicine Berlin (Germany), Europe’s largest university clinic. In addition, the internal guidelines of the Clinic for Orthopaedics and Surgical Orthopaedics of the University Medicine Greifswald (Germany), in co-operation with the clinic for Cardiology, Angiology, Pneumology/Infectiology and Internal Intensive Care Medicine of the University Medicine Greifswald, and the Institute for Hygiene and Environmental Medicine of the University Medicine Greifswald, were considered in this article. An additional expert opinion was obtained from the Adult Reconstruction and Joint Arthroplasty Service of the Hospital for Special Surgery, New York , USA, as part of the epicentre of the COVID-19 pandemic in the western world.
In cases of non-evident or non-existing literature results, considering the rapidly developing situation, our personal clinical recommendations and experiences were given, based on an internal consensus.
Results
The results are divided into the following parts: 1) Recommendations for clinical practice in the current pandemic; 2) Admission screening and procedure for elective and emergency cases; 3) Recommendations for COVID-19-free area of the hospital; 4) Recommendations for the confirmed COVID-19 area of the hospital; 5) Anesthesiologic care of COVID-19 patients; 6) Surgical care of suspected or confirmed COVID-19 patients; and 7) Surgical care of elective non-COVID-19 patients.
1. Recommendations for clinical practice in the current pandemic
In the current pandemic, it is necessary to practice distancing and reduce personal contact as much as possible to reduce the possibility of infection of hospital staff and patients and ultimately disrupt the spread of COVID-19. During the acute phase of COVID-19 it is advised that all non-essential inpatient surgical procedures, including the majority of all elective orthopaedic procedures, should be postponed.9 Outpatient clinics should also reduce their capacity and only treat urgent cases. This reserves resources, including beds and hospital staff, for the treatment of COVID-19 patients.10 The postponement of all elective surgeries is also supposed to reduce the number of patients and thus the risk of uncontrolled spread of COVID-19 within the hospital. Besides, the additional hospital bed capacities are necessary to ensure the special separation into three isolations areas within the hospital: for infected COVID-19 patients, patients with uncertain infection status and non-infected patients (Figure 1).
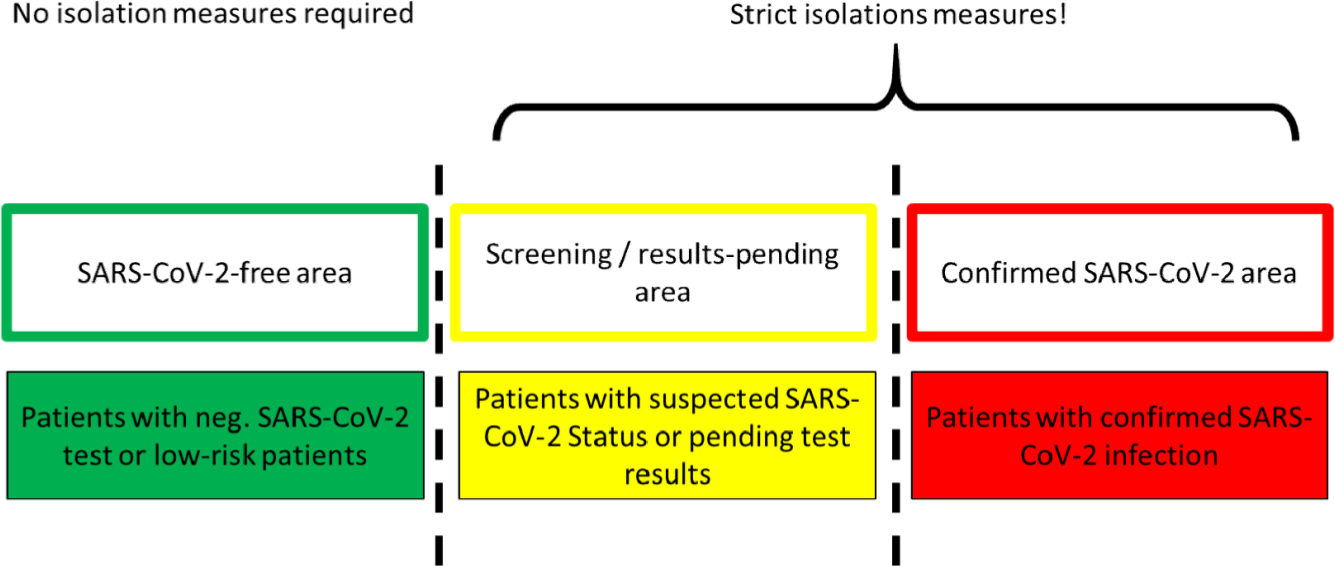
Fig. 1
Division of the hospital into three separate areas for patients with negative, uncertain and positive COVID-19 status. Patients are classified as uncertain in the presence of fever, flu-like symptoms, coughing, throat soreness, fever chills, contact with other COVID-19 patients, or while waiting for their screening test results.
2. Admission screening and procedure for elective and emergency cases
A special admission screening must be established and strictly adhered to prevent infection of clinic personnel and to avoid uncontrolled spreading of COVID-19 within the hospital. This screening is required for all hospital admissions, independently of elective or emergent nature, and should be performed in a separate screening area of the hospital (Figure 2).11 Patients are additionally assessed according to patient history (travel to high-risk areas, contact to COVID-19 patients, employment in medical institutions, nursing homes, or other high-risk institutions) and clinical symptoms, under special consideration of the most common (fever 82% to 87%, coughing 37% to 44%, anosmia 19% to 59%)12,13 and severe ones (dyspnea).13–15 In the presence of any amnestic factors or clinical symptoms, a COVID-19 test should be performed via a combined nose-throat swab (PCR) and in the presence of any clinical symptoms a low-dose CT-scan of the thorax is recommended.16

Fig. 2
Organization and admittance procedure of an orthopaedic/trauma department.
In the case of COVID-19, IgM class antibodies can only be detected after ive to seven days in symptomatic patients, while in asymptomatic or immunosuppressed one’s detection might even be later or not possible at all.17 For that reason, PCR has been used as a direct tool of virus conformation in acute cases, antibody tests as a screening tool for prior contacts and possible existing immunization. Subsequently, antibody tests were also used to test medical staff,18 which then, in case of a possible immunization, could be used in risk areas (COVID-19 patients, suspected cases, emergency rooms). However, up to this date, the exact length and extent of immunity following a first contact remain unknown. Given the high rate of false negative test results, a negative PCR should be repeated in cases of high clinical suspicion.19
For patients presenting with elective/non-life-threatening conditions, in which it is medically justifiable to postpone treatment until the results of a COVID-19 test are present, the screening procedure is performed in the screening area and treatment, if feasible, can be initiated within the same treatment area.Patients presenting with life-threatening conditions, requiring emergency treatment, are admitted directly to the confirmed COVID-19 area of the hospital, enabling a possible immediate therapy. As soon as stabilization of the patient has been successful and life treating events are excluded, an immediate test should be performed. After the test results have been obtained, the patients are transferred to the applicable area of the hospital.20
3. Recommendations for COVID-19-free area of the hospital
The operating procedure in the COVID-19-free area of the hospital is concordant with general hospital and hygiene procedures, with only a few specific recommendations.
All patients and hospital staff within the COVID-19-free area of the hospital have been negatively screened or tested for COVID-19 infection. This can only be guaranteed as long as all hospital personnel and patients are continuously monitored and also self-report any suspicious symptoms. In the absence of clinical symptoms all hospital staff should be tested for COVID-19 infection on a biweekly basis. The clinical re-evaluation of patients is performed by physicians as well as nursing staff. In the presence of any new risk factors or clinical symptoms a new COVID-192 test should be performed.16 This continuous monitoring within the COVID-19-free area intends to immediately identify patients with a new infection, false-negative initial test results, and patients within the incubation period, which is reported to be as long as 14 days.21 The sensitivities and specificities of COVID-19 screening tests cannot be finally assessed due to the limited data available at this point. Preliminary studies report diagnostic sensitivities ranging from 80% to 95%.21,22
Based on the CDC (Centre for Disease Control and Prevention) recommendations, surgical face masks were used to reduce the discharge of aerosols from expiratory air and the radii for contagion (https://www.cdc.gov).23 Every patient admitted to the hospital should be considered a potential carrier of COVID-19, until a negative test result has been obtained, and should receive a surgical face mask upon admittance to the hospital, regardless of admittance to the emergency room, outpatient clinic or as an inpatient. Surgical face masks should also be worn by all persons in the hospital irrespective of visitor or personnel.23
Hand hygiene is an important factor in stopping the spread of COVID-19 and should be practiced upon entering and leaving the hospital, as well as after every contact with patients or potentially contagious surfaces. All alcohol-based disinfectants with the declaration “partially viricidal” are potent against coronaviruses, including COVID-19.3 To facilitate a high compliance, additional disinfectant dispensers should be placed in every patient room, at the hospital entrance, in outpatient clinics and on patient wards.
4. Recommendations for the confirmed COVID-19 area of the hospital
The isolations measures in the confirmed COVID-19 area of the hospital are extensive and necessitate certain structural requirements and special training of all hospital staff at regular intervals by the hygiene department. Apart from guaranteeing the correct hygiene procedures, regular contact with hygiene specialists enables staff a chance to ask questions and propose improvements. All hospital staff involved in the direct care of COVID-19 should also be tested for infection on a weekly basis independently of the presence of clinical symptoms.
The most important structural requirement is the creation of specific anterooms adjacent to every patient room, operating room (OR) or other areas for the treatment of COVID-19 patients. The anterooms are required for the dressing and undressing of personal protective equipment (PPE) (Figure 3 and 4). Multiple confirmed COVID-19 positive patients may be grouped within in a single room as long as proper hygienic procedure can be guaranteed between individual patients. The number and duration of contacts between patients and hospital staff should thereby be reduced to a minimum.24,25 Nursing staff and physicians caring for COVID-19patients should, if possible, only treat COVID-19-positive patients. Additionally, every patient should receive education and instructions concerning isolation protocol, safety measures and proper hand disinfection procedure.26 Patients are only allowed to contact and communicate with friends and family members via mobile telephone, tablet or laptop.
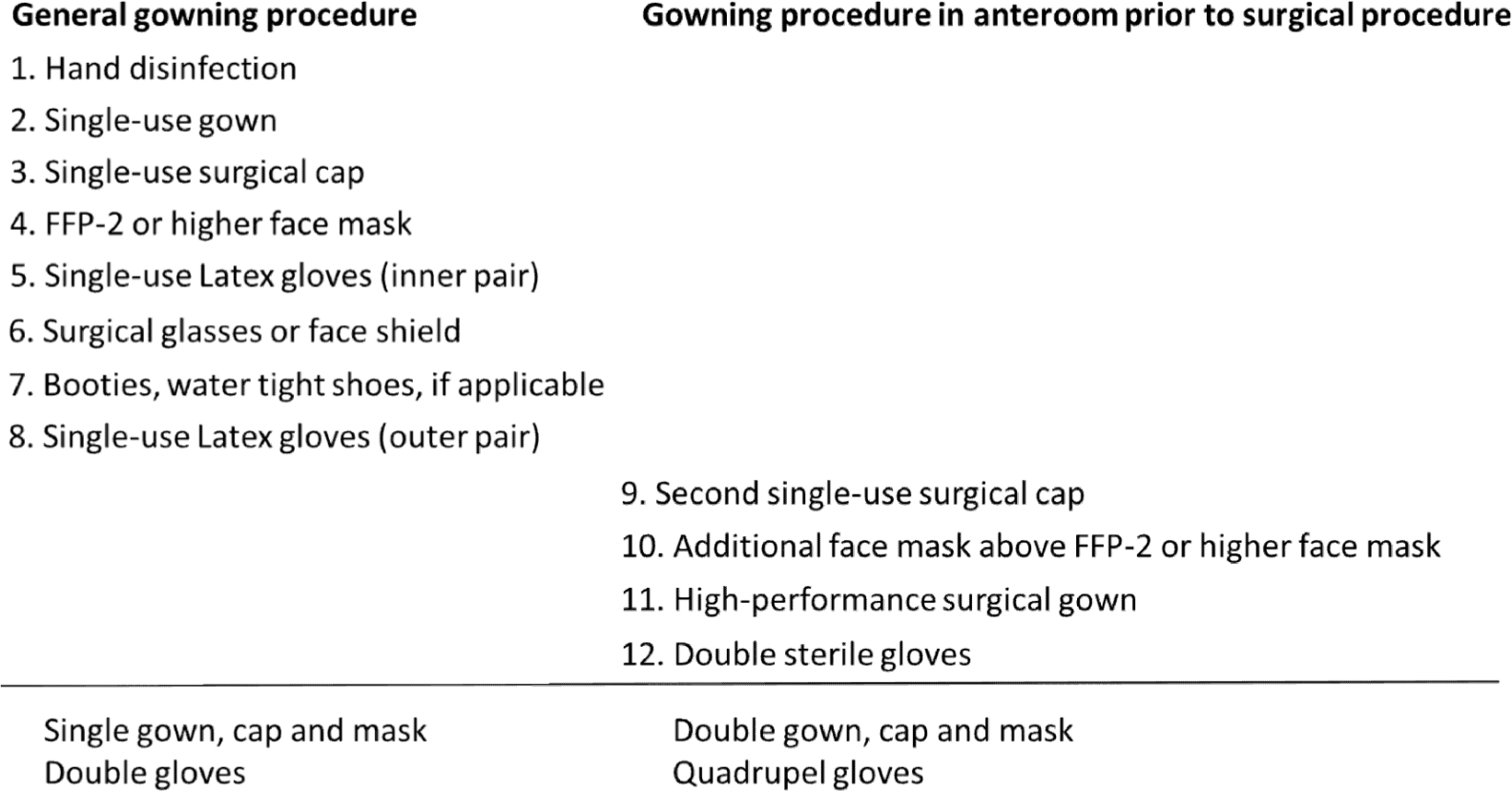
Fig. 3
Proper gowning order for personal protective equipment.

Fig. 4
Proper de-gowning order for personal protective equipment.
5. Anesthesiologic care of COVID-19 patients
The clinical course of COVID-19 can be very dynamic and present with rapid deterioration of the patient’s respiratory, cardiovascular or general condition. Therefore, all symptomatic COVID-19 patients should be monitored continually for their respiratory and cardiovascular function. If the patient’s oxygen saturation drops < 94%, supplemental oxygen therapy is indicated. Advanced monitoring is indicated if the patient’s general condition deteriorates, especially in the presence of somnolence, delirium, dyspnea or reductions in oxygen saturation. Advanced monitoring should include monitoring of oxygen saturation, respiratory frequency, blood pressure and pulse frequency, complete blood count (CBC), C-reactive protein (CRP), D-Dimer, Ferritin, PCT, Interleukin-6 (IL-6), renal and hepatic panel, and a thoracic CT-scan. The following criteria should be reasons for a transfer to the intensive care unit (ICU): respiratory frequency > 30/minutes, oxygen saturation < 93% at rest despite supplemental oxygen therapy, arterial partial pressure of oxygen (PaO2)/inspiratory oxygen concentration (FiO2) < 300 mmHg and radiological progression of pulmonary lesions > 50% within 24 to 48 hours.27
6. Surgical care of suspected or confirmed COVID-19 patients
Isolated reports of viremia in COVID-19 patients are present, thus a blood-borne contagion is theoretically possible, posing the risk of transmission for all OR personnel.28,29 The risk for VOVID-19 transmission is especially increased during orthopaedic and traumatological surgeries due to the development of aerosols from blood, bone, and tissue from hammer blows or powered instruments.30 Therefore, the indications for the surgical care of COVID-19 patients should be made restrictively (life-sustaining operations, mobilization) and in consent with internal medicine and anesthesiology departments. Besides, the quickest or least invasive procedures should be selected.
a) Air exchange systems in operating rooms
Modern ORs are equipped with laminar air flow (LAF) and positive pressure systems reducing the risk of postoperative surgical site infections by directing all air flow away from the patient and channeling all airborne contaminants outside of the OR. In the case of airborne transmission, such as COVID-19, these ventilations systems pose a significant risk of contagion for all hospital personnel. There is limited evidence concerning the risk of COVID-19 contagion in relation to the OR air exchange systems. However, after a careful risk-benefit analysis and consideration of expert opinions the authors recommend the following:
-
If the air from the OR is channeled directly outside of the OR and not into the adjacent rooms, the OR can be used without restriction and standard PPE for the OR staff is sufficient.
-
Negative pressure ORs are preferred for the care of COVID-19 patients.31 If possible, the ventilation system of the OR should be switched from positive to negative pressure. However, even in negative pressure ORs an exchange with the air of neighboring areas occurs as soon as the doors to the OR are opened. Therefore, all doors must remain closed as long as the OR is in use.
-
Class 1a ORs with LAF have a significantly higher volume of air exchange and are preferential to ORs with mixed or turbulent displacement air flow (class 1b), due to the quicker dilution and elimination of aerosols. The unidirectional air flow in ORs with LAF offers additional safety for the OR staff in comparison to the turbulent displacement in class 1b ORs.
-
Class 1b ORs are permitted for orthopaedic and traumatological operations, but are associated with an increased risk of contagion from aerosols, due to the lower volume and turbulent displacement of exchanged air. For this reason, FFP3 masks or positive pressure body exhaust suits should be worn by all personnel in these ORs.32,33
-
All other ORs without air exchange systems, without sterile air filters and low volumes of air exchange, should not be used for the care of SARS-CoV-2 patients, since the aerosols resulting from orthopaedic and traumatological operations are not diluted and high concentrations of aerosols are transferred to the surrounding ambient air once the OR doors are opened.
b) Anteroom and OR procedure
-
Personnel not relevant to the surgical procedure are prohibited from entering the OR. The mobile nurse remains in the sterile hallway and is responsible for delivering the materials relevant to the surgical procedure. The preparation of all operative tables and trays should be performed in the sterile hallway outside of the OR. The OR and the anteroom must remain sealed off from the hallway and remaining areas of the hospital for the duration of the surgical procedure.34
-
The anesthesiologic preparations including induction and recovery are to be performed in a separate area, outside of the OR and the normal induction area. Only the anesthesiology nurse and physician should be present. Specially trained anesthesiology teams should perform the induction and emergence of general anesthesia for COVID-19 patients.35
-
After completion of the operative procedure the OR should be disinfected with an agent of limited viricidal activity, such as oxygen donors, e.g. Descogen liquid.
c) Electrocautery use
The effect of electrocautery smoke in the OR on the infection risk of OR personnel with COVID-19 is currently unknown. However, electrocautery should be omitted or utilized in conjunction with a smoke suction system to prevent the rising of warm air from the surgical field and reduce overall air turbulence within the OR.36
d) Personal protection equipment (PPE) in the OR
PPE is indispensable for self-protection. However, previous experience from Ebola outbreaks has shown, that the efficacy of PPE can only be guaranteed if the dressing and undressing procedure are performed properly (Figure 3 and 4).37 It is highly recommended to have members of the hygiene department demonstrating proper technique. In addition to the general PPE, outside of the OR, specific OR PPE consists of a high-performance gown, double gloves, glasses, and/or face shield and FFP2 or higher surgical face mask (Figure 3 and 4).38
7. Surgical care of elective non-COVID-19 patients
Elective cases must continue at a certain point, given the risk of chronification and reduced outcome following immobilization, muscle atrophy, joint stiffening, pain chronification and even depression. However, surgical treatment is subject to the constraints of current resources and continued compliance with the hygienic precautions.39 Elective surgical treatment occurs within the COVID-19-free areas of the hospital and postoperative care in the outpatient clinics. The gradual return to elective surgery at the author’s departments were planned under consideration of the current national and local infection numbers and epidemiological development.40 The current capacity for elective surgery for the upcoming week was discussed and consented upon by all operative specialties under the coordination of the anesthesiology department. The first patients scheduled for elective surgery should not require postoperative ICU-capacities and the absolute number should be well below the maximum bed capacity of the hospital to ensure the continued adherence to hygienic protocol and allow sufficient capacity for an unexpected admission of new COVID-19 patients. To account for the incubation period of up to 14 days,21 a self-imposed quarantine of the identical duration is recommended to each patient scheduled prior to hospital admission for elective surgery. We consider the combination of a preoperative quarantine period of 14 days and a COVID-19 test a practicable exclusion option for an infection.
Conclusion
The goal of the current social lockdown and restrictions placed upon the healthcare system during this pandemic is to slow the contagion of COVID-19. These measures are necessary to keep the absolute number of COVID-19 patients within the capacity of the health care system. Our guidelines recommend all emergency cases to be treated as COVID-19-positive until proven otherwise. Elective cases should not be postponed indefinitely. Operative roms require structural modifications and specialized PPE for the care of COVID-19 patients, due to the significantly increased risk of contagion during the surgical care. Both patients and medical personnel should regularly be educated on hygiene and correct use of protection equipment. It is unknown when the COVID-19 situation will end or if a recurrence is likely. Without a vaccine, proper hygiene and isolation measures are the only evident strategies. The German concept presented in this article might be useful for further research, especially when comparing the approaches of different countries during the COVID-19 pandemic in the field of orthopaedics.
References
1. Zou L , Ruan F , Huang M , et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients . N Engl J Med . 2020 ; 382 ( 12 ): 1177 – 1179 . Crossref PubMed Google Scholar
2. Kampf G , Todt D , Pfaender S , Steinmann E . Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents . J Hosp Infect . 2020 ; 104 ( 3 ): 246 – 251 . Crossref PubMed Google Scholar
3. Kramer A , Schwebke I , Kampf G . How long do nosocomial pathogens persist on inanimate surfaces? A systematic review . BMC Infect Dis ; 2006 ( 6 ): 130 . Crossref PubMed Google Scholar
4. van Doremalen N , Bushmaker T , Morris DH , et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1 . N Engl J Med . 2020 ; 382 ( 16 ): 1564 – 1567 . Crossref PubMed Google Scholar
5. Bai Y , Yao L , Wei T , et al. Presumed Asymptomatic Carrier Transmission of COVID-19 [published online ahead of print, 2020 Feb 21] . JAMA . 2020 ; 323 ( 14 ): 1406 – 1407 . 10.1001/jama.2020.2565 . Google Scholar
6. Zhang M , Zhou M , Tang F , et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China . J Hosp Infect . 2020 ; 105 ( 2 ): 183 – 187 . Crossref PubMed Google Scholar
7. Li YK , Peng S , Li LQ , et al. Clinical and Transmission Characteristics of Covid-19 - A Retrospective Study of 25 Cases from a Single Thoracic Surgery Department . Curr Med Sci . 2020 ; 40 ( 2 ): 295 – 300 . Crossref PubMed Google Scholar
8. Chu J , Yang N , Wei Y , et al. Clinical characteristics of 54 medical staff with COVID-19: A retrospective study in a single center in Wuhan, China . J Med Virol . 2020 ; 92 ( 7 ): 807 – 813 . Crossref PubMed Google Scholar
9. Chhabra HS , Bagaraia V , Keny S , et al. COVID-19: Current Knowledge and Best Practices for Orthopaedic Surgeons [published online ahead of print, 2020 May 18] . Indian J Orthop . 2020 : 1 – 15 . Google Scholar
10. Randelli PS , Compagnoni R . Management of orthopaedic and traumatology patients during the Coronavirus disease (COVID-19) pandemic in northern Italy . Knee Surg Sports Traumatol Arthrosc . 2020 ; 28 ( 6 ): 1683 – 1689 . Crossref PubMed Google Scholar
11. Kumar A , Kumar A , Das S . Perioperative COVID-19 testing of orthopedic patients: Current evidence [published online ahead of print, 2020 May 12] . J Clin Orthop Trauma . 2020 ; 11 ( Suppl 3 ): S296 – S297 . 10.1016/j.jcot.2020.04.031 . Google Scholar
12. Zhu J , Ji P , Pang J , et al. Clinical characteristics of 3,062 COVID-19 patients: a meta-analysis [published online ahead of print, 2020 Apr 15] . J Med Virol . 2020 . Google Scholar
13. Li J-Y , You Z , Wang Q , et al. The epidemic of 2019-novel-coronavirus (2019-nCoV) pneumonia and insights for emerging infectious diseases in the future . Microbes Infect . 2020 ; 22 ( 2 ): 80 – 85 . Crossref PubMed Google Scholar
14. Wynants L , Van Calster B , Collins GS , et al. Prediction models for diagnosis and prognosis of covid-19 infection: systematic review and critical appraisal [published correction appears in BMJ. 2020 Jun 3;369:m2204] . BMJ . 2020 ; 369 : m1328 . Google Scholar
15. Cheng ZJ , Shan J . 2019 Novel coronavirus: where we are and what we know . Infection . 2020 ; 48 ( 2 ): 155 – 163 . Crossref PubMed Google Scholar
16. Ai T , Yang Z , Hou H , et al. Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases [published online ahead of print, 2020 Feb 26] . Radiology . 2020 : 200642 . Google Scholar
17. Jacofsky D , Jacofsky EM , Jacofsky M . Understanding Antibody Testing for COVID-19 [published online ahead of print, 2020 Apr 27] . J Arthroplasty . 2020 : S0883-5403(20)30442-3 . Google Scholar
18. Yan Y , Chang L , Wang L . Laboratory testing of SARS-CoV, MERS-CoV, and SARS-CoV-2 (2019-nCoV): Current status, challenges, and countermeasures . Rev Med Virol . 2020 ; 30 ( 3 ): e2106 . Crossref PubMed Google Scholar
19. Pascarella G , Strumia A , Piliego C , et al. COVID-19 diagnosis and management: a comprehensive review [published online ahead of print, 2020 Apr 29] . J Intern Med . 2020 . Google Scholar
20. Service BC , Collins AP , Crespo A , et al. Medically Necessary Orthopaedic Surgery During the COVID-19 Pandemic: Safe Surgical Practices and a Classification to Guide Treatment [published online ahead of print, 2020 May 13] . J Bone Joint Surg Am . 2020 . 10.2106/JBJS.20.00599.10.2106/JBJS.20.00599 . Google Scholar
21. Kokkinakis I , Selby K , Favrat B , Genton B , Cornuz J . Performance du frottis nasopharyngé-PCR pour le diagnostic du Covid-19 - Recommandations pratiques sur la base des premières données scientifiques [Covid-19 diagnosis : clinical recommendations and performance of nasopharyngeal swab-PCR] . Rev Med Suisse . 2020 ; 16 ( 689 ): 699 – 701 . Google Scholar
22. Corman VM , Landt O , Kaiser M , et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR . Euro Surveill . 2020 ; 25 ( 3 ): 2000045 . Crossref PubMed Google Scholar
23. Offeddu V , Yung CF , Low MSF , Tam CC . Effectiveness of Masks and Respirators Against Respiratory Infections in Healthcare Workers: A Systematic Review and Meta-Analysis . Clin Infect Dis . 2017 ; 65 ( 11 ): 1934 – 1942 . Crossref PubMed Google Scholar
24. Massey PA , McClary K , Zhang AS , Savoie FH , Barton RS . Orthopaedic Surgical Selection and Inpatient Paradigms During the Coronavirus (COVID-19) Pandemic . J Am Acad Orthop Surg . 2020 ; 28 ( 11 ): 436 – 450 . Crossref PubMed Google Scholar
25. Huang L , Lin G , Tang L , Yu L , Zhou Z . Special attention to nurses' protection during the COVID-19 epidemic . Crit Care . 2020 ; 24 ( 1 ): 120 . Crossref PubMed Google Scholar
26. Gibson Miller J , Hartman TK , Levita L , et al. Capability, opportunity, and motivation to enact hygienic practices in the early stages of the COVID-19 outbreak in the United Kingdom [published online ahead of print, 2020 May 16] . Br J Health Psychol . 2020 . Google Scholar
27. Wujtewicz M , Dylczyk-Sommer A , Aszkiełowicz A , et al. COVID-19 - what should anaethesiologists and intensivists know about it? Anaesthesiol Intensive Ther . 2020 ; 52 ( 1 ): 34 – 41 . Crossref PubMed Google Scholar
28. Chang L , Yan Y , Wang L , Disease C . 2019: coronaviruses and blood safety . Transfus Med Rev . 2020 ; 34 ( 2 ): 75 – 80 . Google Scholar
29. Wang W , Xu Y , Gao R , et al. Detection of SARS-CoV-2 in Different Types of Clinical Specimens [published online ahead of print, 2020 Mar 11] . JAMA . 2020 ; 323 ( 18 ): 1843 – 1844 . 10.1001/jama.2020.3786 . Google Scholar
30. Basso T , Dale H , Langvatn H , et al. Virus transmission during orthopedic surgery on patients with COVID-19 - a brief narrative review [published online ahead of print, 2020 May 14] . Acta Orthop . 2020 : 1 – 4 . Google Scholar
31. Awad ME , Rumley JCL , Vazquez JA , Devine JG . Perioperative Considerations in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic Patients: Operating Room Protocols and Recommendations in the Current COVID-19 Pandemic . J Am Acad Orthop Surg . 2020 ; 28 ( 11 ): 451 – 463 . Crossref PubMed Google Scholar
32. Carli AV . CORR Insights®: Surgeon Personal Protection: An Underappreciated Benefit of Positive-pressure Exhaust Suits . Clin Orthop Relat Res . 2018 ; 476 ( 6 ): 1349 – 1351 . Crossref PubMed Google Scholar
33. Makovicka JL , Bingham JS , Patel KA , et al. Surgeon Personal Protection: An Underappreciated Benefit of Positive-pressure Exhaust Suits . Clin Orthop Relat Res . 2018 ; 476 ( 6 ): 1341 – 1348 . Crossref PubMed Google Scholar
34. Rodrigues-Pinto R , Sousa R , Oliveira A . Preparing to Perform Trauma and Orthopaedic Surgery on Patients with COVID-19 . J Bone Joint Surg Am . 2020 ; 102 ( 11 ): 946 – 950 . Crossref PubMed Google Scholar
35. Cook TM , El-Boghdadly K , McGuire B , et al. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists . Anaesthesia . 2020 ; 75 ( 6 ): 785 – 799 . Crossref PubMed Google Scholar
36. Alp E , Bijl D , Bleichrodt RP , Hansson B , Voss A . Surgical smoke and infection control . J Hosp Infect . 2006 ; 62 ( 1 ): 1 – 5 . Crossref PubMed Google Scholar
37. Casanova LM , Erukunuakpor K , Kraft CS , et al. Assessing Viral Transfer During Doffing of Ebola-Level Personal Protective Equipment in a Biocontainment Unit . Clin Infect Dis . 2018 ; 66 ( 6 ): 945 – 949 . Crossref PubMed Google Scholar
38. Hirschmann MT , Hart A , Henckel J , et al. COVID-19 coronavirus: recommended personal protective equipment for the orthopaedic and trauma surgeon [published correction appears in Knee Surg Sports Traumatol Arthrosc. 2020 Jun 12;:] . Knee Surg Sports Traumatol Arthrosc . 2020 ; 28 ( 6 ): 1690 – 1698 . 10.1007/s00167-020-06022-4 . Google Scholar
39. Mouton C , Hirschmann MT , Ollivier M , Seil R , Menetrey J . COVID-19 - ESSKA guidelines and recommendations for resuming elective surgery . J Exp Orthop . 2020 ; 7 ( 1 ): 28 . Crossref PubMed Google Scholar
40. Collaborative C . Elective surgery cancellations due to the COVID-19 pandemic: global predictive modelling to inform surgical recovery plans [published online ahead of print, 2020 May 12] . Br J Surg . 2020 . Google Scholar
Author contributions
M. Müller: Idea and conceptulization, Wrote the manuscript, including literature review, Carried out revision and resubmission.
F. Boettner: Wrote the manuscript, including literature review, Offered special expert counseling.
D. Karczewski: Wrotethe manuscript, including literature review, Undertook submission and language corrections, Carried out revision and resubmission.
V. Janz: Wrote the manuscript, including literature review.
S. Felix: Wrote the manuscript, including literature review, Offered special expert counseling.
A. Kramer: Wrote the manuscript, including literature review, Offered special expert counseling.
G. I. Wassilew: Idea and conceptulization, Wrote the manuscript, including literature review.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
