




Abstract
Introduction
Studies have addressed the issue of increasing prevalence of work-related musculoskeletal (MSK) pain among different occupations. However, contributing factors to MSK pain have not been fully investigated among orthopaedic surgeons. Thus, this study aimed to approximate the prevalence and predictors of MSK pain among Saudi orthopaedic surgeons working in Riyadh, Saudi Arabia.
Methods
A cross-sectional study using an electronic survey was conducted in Riyadh. The questionnaire was distributed through email among orthopaedic surgeons in Riyadh hospitals. Standardized Nordic questionnaires for the analysis of musculoskeletal symptoms were used. Descriptive measures for categorical and numerical variables were presented. Student’s t-test and Pearson’s χ2 test were used. The level of statistical significance was set at p ≤ 0.05.
Results
The response rate was 80.3%, with a total number of 179 of Saudi orthopaedic surgeons (173 males and six females). Of our sample, 67.0% of the respondents complained of having MSK pain. The most commonly reported MSK pain was lower back (74.0%), followed by neck (58.2%). Age and body mass index were implicated in the development of more than one type of MSK pain. Increased years of experience (≥ 6 years) was linked to shoulder/elbow, lower back, and hip/thigh pain. Smoking is widely associated with lower back pain development, whereas physicians who do not smoke and exercise regularly reported fewer pain incidences. Excessive bending and twisting during daily practice have been correlated with increased neck pain.
Conclusion
MSK pain was found to be common among Saudi orthopaedic surgeons. Further extensive research should be conducted to understand and analyze the risk factors involved and search for possible improvements to avoid further complications. However, ergonomics education during surgical training could be effective at modifying behaviors and reducing MSK pain manifestations.
Introduction
Work-related musculoskeletal (MSK) pain is common among practitioners in the medical, surgical, and dental communities.1,2 Surgeons, more commonly those specialized in orthopedics, are more prone to MSK pain during their practice.3 MSK pain among orthopaedic surgeons is attributed to physiological and ergonomic factors. Predictors such as prolonged physical activity, longer working hours, repetitive movements when using tools, and awkward positions during surgery is associated with MSK pain.4,5 Such predictors commonly affect the back, neck, and upper limbs.6,7
Among members of the Paediatric Orthopaedic Society of North America, 67% reported a work-related MSK pain.8 Alqahtani et al. showed that practice-related MSK pain affects 66% of arthroplasty surgeons and 67% of trauma orthopaedic surgeons.9,10 However, a lower prevalence of 44% among orthopaedic surgeons was reported by Davis et al.7 Nevertheless, the prevalence of MSK pain among healthcare providers in Saudi Arabia ranged between 48% and 85%.1,11-13
However, to our knowledge, no study has shown the prevalence, consequences, and risk factors of MSK pain among orthopaedic surgeons in Saudi Arabia. Thus, this study aimed to estimate the prevalence of MSK pain and its possible complications among orthopaedic surgeons who work at Riyadh hospitals and to identify the risk factors of developing MSK pain and its significant predictors.
Methods
Study population
This cross-sectional study was conducted in Riyadh, Saudi Arabia, using online-based survey. There are approximately 415 government hospitals and 127 private hospitals in Saudi Arabia; 270 of them are under the umbrella of the Ministry of Health. The number of orthopaedic surgeons in Saudi Arabia reaches up to 2179. Of them, only 411 work in Riyadh. The majority of 224 orthopaedic surgeons working in Riyadh are Saudi, while the rest of 187 are non-Saudi. The questionnaire was submitted to 224 Saudi orthopaedic surgeons in Riyadh. Data were collected between February and April 2018. Male and female Saudi orthopaedic surgeons who worked for at least one year were included in the study. All orthopaedic surgeons with congenital deformities or history of trauma that may affect their MSK functions were excluded.
According to the prevalence of 67% reported by Alqahtani et al,9 the input data used with a confidence interval (two-sided) of 95%, and 0.05 absolute precision, the appropriate sample size equals to 136. However, to overcome an average of 10% of no response or incomplete surveys, a sample size of 150 orthopaedic surgeons was considered. However, the total population was not that much bigger than the calculated sample, and so the authors decided to submit the survey to all 224 Saudi surgeons in Riyadh. Surprisingly, the response rate was 80.3%, which is 125% higher than that wanted during the study time (Figure 1). The total number of participants was 180; however, one was excluded due to a history of obstetric brachial plexus palsy, which recovered spontanously.14
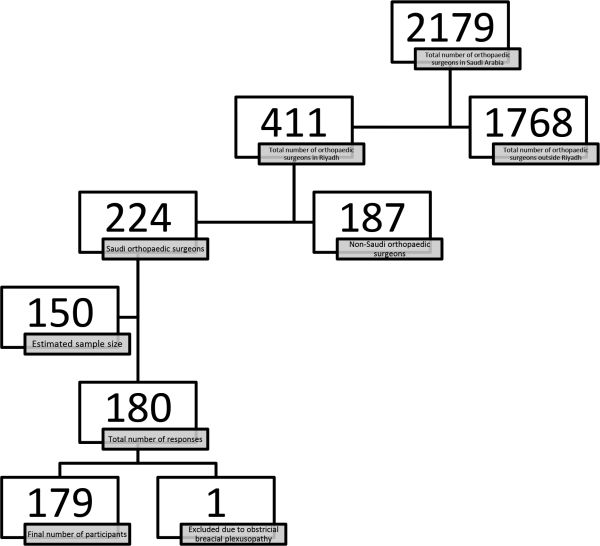
Figure 1
Flow diagram of the study participants.
Survey
The questionnaire was previously used in the existing literature.15 The questionnaire underwent meticulous revision to further fulfill the objectives of the study. No major changes affecting the validity or reliability of the survey were made, and the questionnaire was administered in English. The questionnaire had two main domains: the first domain is built mainly to cull sociodemographic data of the study respondents, while the other domain pooled information about the symptoms of MSK pain over the past year. Other data concerning the burden of MSK pain on work were also gathered such as seeking medical help, quitting the job, and workdays lost. An email with the study questionnaire was sent to every subject meeting the inclusion criteria. Reminders were planned to be sent if the responses were not adequate.
Measures
Pain severity was assessed by using 0 to 10 numeric rating scale: a score range of 0 to 4 was considered mild pain, a score of 5 to 7 was considered moderate pain, and a score of 8 to 10 was considered severe pain.16
Statistical analysis
All statistical analyses were performed using SPSS Statistics for Mac version 22.0 (IBM, Armonk, New York, USA). Categorical variables were presented as frequencies and percentages, whereas continuous variables were summarized as the mean ± standard deviation or medians and centiles when distributions were skewed. Prevalence was calculated by dividing the number of participants who had a symptom outcome by the total number of participants. Student’s t-test and independent samples t-test were used to compare the sample means. Categorical data were analyzed using Pearson’s χ2 test. Multivariate logistic regression for categorical variables was performed to assess the significant factors with adjustment for confounding factors such as age. The p-value was set at 0.05 for all tests applied.
Results
Sociodemographic characteristics
Among participants (179) who completed the survey, 96.6% were male (mean age 32.2 years ( ± 7.7); 24.0 and 66.0) and 101 participants (56.4%) were married. The mean body mass index (BMI) of the participants was 27.8 ( ± 5.2) kg/m2. In all, 66 (36.9%) of the participants are smokers, and 92 participants (51.4%) reported participating in exercise and sports.
In addition, 167 (93.3%) of the responders were right-handed. The median years of experience for both sexes was five years with the midspread range of one to nine years. The sample consisted of 43 consultants (24%) and 26 (14.5%) fellows/assistant/associate consultants, while the rest were residents with different levels of training.
Furthermore, 151 (84.4%) of the participants reported excessive bending or twisting for better access during surgeries and physical examinations, and 120 (67.0%) of the participants experienced MSK pain. Table I summarizes all baseline qualities of the orthopaedic surgeons who participated in the study.
Table I.
Baseline characteristics of study participants.
| Categories | Variable |
|---|---|
| Age (years), mean (± SD), range | 32.2 (± 7.7), 24.0 to 66.0 |
| Sex , n (%) | |
| Female | 6 (3.4) |
| Male | 173 (96.6) |
| Marital status, n (%) | |
| Single | 78 (43.6) |
| Married | 101 (56.4) |
| Private practice (n %) | |
| No | 196 (94.4) |
| Yes | 10 (5.6) |
| Sub-specialty, n (%) | |
| General | 128 (71.5) |
| Paediatrics | 16 (8.9) |
| Upper limb | 6 (3.4) |
| Arthroplasty | 9 (5) |
| Sport | 4 (2.2) |
| Foot and ankle | 3 (1.7) |
| Trauma | 10 (5.6) |
| Spine | 2 (1.1) |
| Oncology | 1 (0.6) |
| BMI, mean (± SD) | 27.8 (5.2) |
| Smoking, n (%) | |
| No | 113 (63.1) |
| Yes | 66 (39.6) |
| Exercising, n (%) | |
| No | 87 (48.6) |
| Yes | 92 (51.4) |
| Handedness, n (%) | |
| Right-handed | 167 (93.3) |
| Left-handed | 12 (6.7) |
| Level, n (%) | |
| Consultant | 43 (24) |
| Fellow, assistant/associate consultant | 26 (14.5) |
| R1 | 19 (10.6) |
| R2 | 31 (17.3) |
| R3 | 22 (12.3) |
| R4 | 21 (11.7) |
| R5 | 17 |
| Years of experience, median (range) | 5 (1 to 9) |
| Bending or twisting for better access, n (%) | |
| No | 28 (15.6) |
| Yes | 151 (84.4%) |
| MSK pain, n (%) | |
| No | 59 (33) |
| Yes | 120 (67) |
-
MSK, musculoskeletal; SD, standard deviation
Prevalence of work-related MSK pain at different body sites
The prevalence of MSK pain was 67.0%. Among those who reported any MSK pain, the highest responses of pain were those of lower back pain, reaching a remarkable prevalence of 74.0%. The second highest reported prevalence was neck pain, making up 58.2% of the reports. Furthermore, 40.4% complained of having shoulder and/or elbow pain. Hand and/or wrist pain was prevalent among 32.2% of the respondents, while knee pain and foot and/or ankle pain composed of 27.4%, 21.2% of the responses respectively. Finally, 11.6% of the respondents experienced hip and/or thigh pain. Figure 2 illustrates the 95% confidence interval (CI) of pain throughout the MSK system.
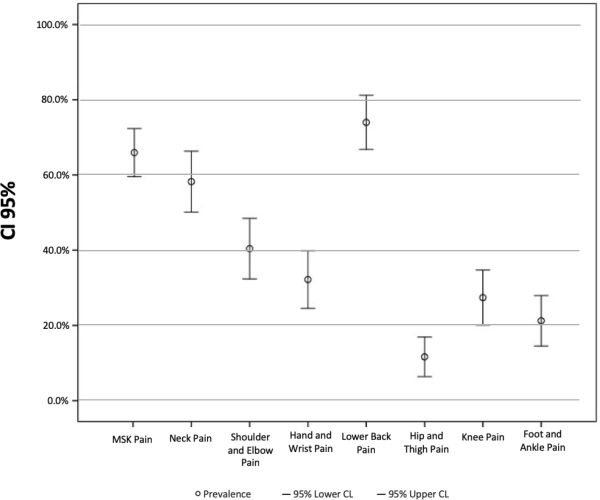
Figure 2
Prevalence of work-related musculoskeletal pain at different body site.
MSK pain characteristics
MSK pain characteristics that were reported by the study participants are shown in Table II. Of the participants, 28.7% reported lower back pain more than five times during the previous year, as did the 22.6% of the sample population who reported neck pain. Different levels of MSK pain severity were reported by the study participants based on body site as well; 75% reported mild neck pain. The vast majority of the sample had no changes in their job as a result of their MSK pain. In addition, during the past year, most did not take any sick leave related to MSK pain. However, only a very few participants took it for more than five times in the past 12 months.
Table II.
Characteristics of different types of musculoskeletal pain.
| Variable(s) | Categories | Neck pain | Shoulder/elbow pain | Hand/wrist pain | Lower back pain | Hip/thigh pain | Knee pain | Foot/ankle pain |
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Duration of pain | Shorter than 4 weeks | 58 (69.0) | 31 (52.5) | 25 (53.2) | 60 (56.1) | 5 (29.4) | 19 (48.7) | 11 (35.5) |
| Between 2 and 3 months | 14 (16.7) | 17 (28.8) | 16 (34.0) | 21 (19.6) | 4 (23.5) | 11 (28.2) | 13 (41.9) | |
| Between 3 and 6 months | 8 (9.5) | 4 (6.8) | 5 (10.6) | 11 (10.3) | 2 (11.8) | 5 (12.8) | 3 (9.7) | |
| Longer than 6 months | 4 (4.8) | 7 (11.9) | 1 (2.1) | 15 (14.0) | 6 (35.3) | 4 (10.3) | 4 (12.9) | |
| Frequency of pain attacks (time period) | < 5 times | 65 (77.3) | 45 (76.3) | 34 (72.4) | 77 (71.3) | 7 (41.2) | 29 (72.5) | 17 (54.9) |
| > 5 times | 19 (22.6) | 14 (23.7) | 13 (27.7) | 31 (28.7) | 10 (58.8) | 11 (27.5) | 14 (45.2) | |
| Sought medical attention | 20 (23.5) | 18 (31.0) | 12 (26.0) | 19 (17.6) | 2 (11.8) | 10 (25.0) | 6 (19.3) | |
| Changed job | 1 (1.2) | 2 (3.4) | 2 (4.3) | 6 (5.6) | 1 (5.9) | 2 (5.1) | 0 (0.0) | |
| Took sick leave in past 12 months | 0 times | 81 (95.3) | 55 (94.8) | 40 (85.1) | 90 (83.3) | 16 (94.1) | 35 (87.5) | 27 (87.1) |
| 1 to 5 times | 4 (4.7) | 3 (5.2) | 6 (12.8) | 15 (13.9) | 0 (0.0) | 4 (10.0) | 3 (9.7) | |
| > 5 times | 0 (0.0) | 0 (0.0) | 1 (2.1) | 3 (2.8) | 1 (5.9) | 1 (2.5) | 1 (3.2) | |
| Intensity of pain (scale of 1 to 10) | Mild (1 to 3) | 63 (75.0) | 46 (78.0) | 29 (61.7) | 35 (32.4) | 12 (70.6) | 27 (67.5) | 19 (63.3) |
| Moderate (4to 7) | 20 23.8) | 12 (20.3) | 16 (34.0) | 63 (58.3) | 4 (23.5) | 11 (27.5) | 9 (30.0) | |
| Severe (8 to 10) | 1 (1.2) | 1 (1.7) | 2 (4.3) | 10 (9.3) | 1 (5.9) | 2 (5.0) | 2 (6.7) | |
Bivariate analysis of MSK pain predictors
No correlation was found between marital status and any type of MSK pain. However, a significant correlation between foot/ankle pain (p = 0.06) and marital status might be found if a bigger population size was included. Only ten of 179 surgeons were working in private clinics. No significant difference was found in any of the pain outcomes between surgeons in private clinics and those who work in government hospitals or clinics (data not shown).
The results also illustrated a correlation between increased BMI levels (30 ± 5.9) and development of knee, and foot/ankle pain. In addition, a relationship was noted between smoking and lower back pain, and hip/thigh pain prevalence. Neck, hip/thigh, and knee pain was more commonly found among doctors who do not exercise or take any part in sports. Predictors of the development of MSK pain were also correlated with age, years of experience, smoking and twisting or bending for better access.
Table III summarizes the entire results of the bivariate regression analysis of MSK pain predictors among orthopaedic surgeons.
Table III.
Association of baseline characteristics and musculoskeletal pain.
| MSK pain | Neck pain | Shoulder/elbow pain | Hand/wrist pain | Lower back pain | Hip/thigh pain | Knee pain | Foot/ankle pain | |
|---|---|---|---|---|---|---|---|---|
| Variables | n = 120 | n = 85 | n = 59 | n = 47 | n = 108 | n = 17 | n = 40 | n = 31 |
| Age, mean (SD) | 32.2 (7.3) | 32 (8.5) | 34.2 (9.0) | 32.2 (7.3) | 32.8 (8.2) | 36.6 (9.6) | 35.4 (10.1) | 33.5 (7.8) |
| p-value | 0.96 | 0.922 | 0.008 | 0.897 | 0.011 | 0.007 | 0.011 | 0.247 |
| Sex, n (%) | ||||||||
| Female | 5 (4.2) | 5 (5.9) | 4 (6.8) | 2 (4.3) | 4 (3.7) | 1 (5.9) | 2 (5.0) | 1 (3.2) |
| Male | 115 (95.8) | 80 (94.1) | 55 (93.2) | 45 (95.7) | 104 (96.3) | 16 (94.1) | 38 (95.0) | 30 (96.8) |
| p-value | 0.388 | 0.054 | 0.066 | 0.704 | 0.755 | 0.553 | 0.52 | 0.945 |
| Marital status n (%) | ||||||||
| Single | 52 (43.3) | 40 (47.1) | 24 (40.7) | 18 (38.3) | 44 (40.7) | 5 (29.4) | 15 (37.5) | 9 (29.0) |
| Married | 68 (56.7) | 45 (52.9) | 35 (59.3) | 29 (61.7) | 64 (59.3) | 12 (70.6) | 25 (62.5) | 22 (71.0) |
| p-value | 0.926 | 0.354 | 0.527 | 0.353 | 0.204 | 0.202 | 0.343 | 0.061 |
| Body mass index, mean (SD) | 28.9 (5.7) | 27.5 (5.1) | 27.6 (5.1) | 28.4 (5.5) | 28.4 (5.7) | 30.9 (7.8) | 30 (5.9) | 29.8 (5.8) |
| p-value | 0.161 | 0.12 | 0.364 | 0.635 | 0.232 | 0.12 | 0.01 | 0.046 |
| Smoking, n (%) | ||||||||
| No | 72 (60.0) | 49 (57.6) | 32 (54.2) | 28 (59.6) | 67 (62.0) | 6 (35.3) | 24 (60.0) | 17 (54.8) |
| Yes | 48 (40.0) | 36 (42.4) | 27 (45.8) | 19 (40.4) | 41 (38.0) | 11 (64.7) | 16 (40.0) | 14 (45.2) |
| p-value | 0.216 | 0.241 | 0.13 | 0.723 | 0.027 | 0.017 | 0.802 | 0.38 |
| Exercising, n (%) | ||||||||
| No | 57 (47.5) | 47 (55.3) | 27 (45.8) | 22 (46.8) | 54 (50.0) | 12 (70.6) | 22 (55.0) | 15 (48.4) |
| Yes | 63 (52.5) | 38 (44.7) | 32 (54.2) | 25 (53.2) | 54 (50.0) | 5 (29.4) | 18 (45.0) | 16 (51.6) |
| p-value | 0.674 | 0.022 | 0.765 | 0.94 | 0.869 | 0.04 | 0.004 | 0.887 |
| Years of experience, mean (SD) | 6.3 (6.2) | 6.6 (7.1) | 8.2 (7.4) | 6.3 (5.8) | 6.8 (6.8) | 10.4 (7.9) | 9.4 (8.6) | 6.7 (6.3) |
| p-value | 0.725 | 0.511 | 0.005 | 0.994 | 0.015 | 0.003 | 0.25 | 0.684 |
| Bending or twisting for better access, n (%) | ||||||||
| No | 13 (10.8) | 7 (8.2) | 8 (13.6) | 6 (12.8) | 13 (12.0) | 3 (17.6) | 6 (15.0) | 2 (6.5) |
| Yes | 107 (89.2) | 78 (91.8) | 51 (86.4) | 41 (87.2) | 95 (88.0) | 14 (82.4) | 34 (85.0) | 29 (93.5) |
| p-value | 0.012 | 0.043 | 0.872 | 0.951 | 0.554 | 0.546 | 0.661 | 0.221 |
| Age bracket, n (%) | ||||||||
| 20 to 30 | 69 (57.5) | 54 (63.5) | 30 (50) | 27 (57.4) | 61 (56.5) | 6 (35.3) | 19 (47.5) | 14 (45.2) |
| 31 to 40 | 35 (29.2) | 19 (22.4) | 17(28.8) | 12 (25.5) | 29 (26.9) | 7 (41.2) | 10 (25) | 12 (38.7) |
| 41 to 50 | 12 (10) | 7 (8.2) | 8 (13.6) | 7 (14.9) | 13 (12) | 3 (17.6) | 7 (17.5) | 4 (12.9) |
| 51 to 60 | 4 (3.3) | 4 (4.7) | 3 (5.1) | 1 (2.1) | 4 (3.7) | 0 (0) | 3 (7.5) | 1 (3.2) |
| 61 to 70 | 0 (0) | 1 (1.2) | 1 (1.7) | 0 (0) | 1 (0.9) | 1 (5.9) | 1 (2.5) | 0 (0) |
| p-value | 0.172 | 0.064 | 0.165 | 0.564 | 0.138 | 0.05 | 0.025 | 0.443 |
| Speciality, n (%) | ||||||||
| General | 82 (68.3) | 61 (71.8) | 38 (64.4) | 31 (66) | 71 (65.7) | 9 (52.9) | 24 (60) | 22 (71) |
| Pediatrics | 12 (10) | 6 (7.1) | 6 (10.2) | 6 (12.8) | 12 (11.1) | 2 (11.8) | 6 (15) | 3 (9.7) |
| Upper limb | 5 (4.2) | 3 (3.5) | 3 (5.1) | 0 (0) | 5 (4.6) | 0 (0) | 3 (7.5) | 1 (3.2) |
| Arthroplasty | 5 (4.2) | 5 (5.9) | 4 (6.8) | 4 (8.5) | 5 (4.6) | 2 (11.8) | 2 (5) | 2 (6.5) |
| Sport | 4 (3.3) | 2 (2.4) | 0 (0) | 1 (2.1) | 4 (3.7) | 0 (0) | 1 (2.5) | 0 (0) |
| Foot and ankle | 2 (1.7) | 0 (0) | 1 (1.7) | 2 (4.3) | 1 (0.9) | 0 (0) | 1 (2.5) | 0 (0) |
| Trauma | 7 (5.8) | 7 (8.2) | 6 (10.2) | 2 (4.3) | 8 (7.4) | 2 (11.8) | 1 (2.5) | 1 (3.2) |
| Spine | 2 (1.7) | 1 (1.2) | 1 (1.7) | 1 (2.1) | 1 (0.9) | 1 5.9) | 1 (2.5) | 1 (3.2) |
| Oncology | 1 (0.8) | 0 (0) | 0 (0) | 0 (0) | 1 (0.9) | 1 (5.9) | 1 (2.5) | 1 (3.2) |
| p-value | 0.438 | 0.387 | 0.304 | 0.085 | 0.304 | 0.137 | 0.326 | 0.46 |
-
MSK, musculoskeletal; SD, standard deviation.
Multivariate analysis
Using logistic regression (Table IV), years of experience did not play a role after adjusting for age in shoulder/elbow, lower back, and hip/thigh pain development. Repetitive bending and flexion to get better approach or visibility during surgery and examination is a significant predictor of MSK pain when adjusting for age, BMI, and exercise engagement (adjusted odds ratio (aOR) = 3.3, p = 0.008; 95% CI 1.3 to 7.9).
Table IV.
Multivariate logistic regression analysis of MSK pain predictors.
| Region | Variable | Category | aOR | 95% confidence interval | P-Value |
|---|---|---|---|---|---|
| MSK pain | BMI | N/A | 1.06 | 0.98 to 1.13 | 0.14 |
| Bending or twisting for better access | Yes | 3.28 | 1.35 to 7.94 | 0.01 | |
| Exercising | Yes | 1.41 | 0.72 to 2.77 | 0.31 | |
| Sex | Male | 0.37 | 0.04 to 3.35 | 0.37 | |
| Neck pain | Exercising | Yes | 0.38 | 0.177 to 0.805 | 0.01 |
| Hip/thigh pain | Smoking | Yes | 6.16 | 1.56 to 24.27 | 0.01 |
| Years of experience | 1.28 | 1.02 to 1.59 | 0.03 | ||
| Foot/ankle pain | Age | 31 to 40 | 3.38 | 1.09 to 10.48 | 0.03 |
| 41 to 50 | 12.68 | 1.23 to 131.11 | 0.03 | ||
| 51 to 60 | 51.01 | 0.59 to 4376.35 | 0.08 | ||
| BMI | 1.10 | 1.01 to 1.20 | 0.03 |
-
aOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; MSK, musculoskeletal.; N/A, not applicable
After adjusting the effect of common related variables of lower back pain, shoulder/elbow pain, and knee pain, age, sex, BMI, practicing exercise, years of experience, and smoking were not significantly associated with having pain in those sites.
Practicing exercise seems to lower the odds of having neck pain even after adjusting for BMI and age (aOR = 0.38, p = 0.01; 95% CI: 0.177 to 0.81). Hip/thigh pain is significantly associated with increased years of experience (OR = 1.28, p = 0.03; 95% CI: 1.02 to 1.59) and to being smoker (OR = 6.16, p = 0.01; 95% CI: 1.56 to 24.27).
BMI was a significant predictor of foot/ankle pain (OR = 1.1, p = 0.03; 95% CI: 1.0 to 1.2), as well as middle ages 31 to 40 years and 41 to 50 years (OR = 3.38 and 12.68; 95% CI: 1.09 to 10.48 and 95% CI: 1.2 to 131.1, respectively).
Discussion
MSK pain among practicing orthopaedic surgeons in Saudi Arabia is a prevalent problem. Lower back and neck pain are the most prevalent sites involved. Age, smoking, BMI, and years of experience were strongly correlated with significant problem.
Orthopaedic surgeons are bombarded with numerous hardships at work, from standing long hours at the operating rooms to awkward body positions during patient examinations. Previous studies have tackled this particular issue and illustrated the growing prevalence of MSK pain among orthopaedic surgeons.17 Wong et al reported that 84.1% of the individuals who reported that pain was due to their current job were orthopaedic surgeons. Moreover, 94.4% of the participants believe that the pain is due to their occupation, and 72.6% reported increased MSK pain from the beginning of their careers.18
MSK pain is common among contributions of several predictors including sex, BMI, smoking habits, years in practice, and posture positions. Compared to the USA, Canada, and India,17,19,20 Saudi Arabia has the highest MSK pain prevalence (67%) among orthopaedic surgeons. Moreover, the present study illustrated that the incidence of neck pain was approximately 58%, which is approximately similar to results reported by previous studies (59%).17 Besides, lower back pain has a prevalence of almost 74% among Saudi Arabian orthopaedic surgeons, which is exceedingly higher than the reported numbers of lower back pain (55%).17 However, MSK pain is more prevalent among Saudi orthopedists in Riyadh (67%) than the general population in Saudi Arabia (25.4%).21 During the study period, 31.2% of the surveyed general population complained of MSK pain.22 Lower incidence of MSK pain among construction workers in Saudi Arabia was also found with 48.5% of workers complaining of MSK pain.23
In our study, the most common MSK-related pain was mainly in the lower back (74%) and neck (58.2%). During surgeries, surgeons constantly look down and bend their neck. Eventually, due to the excessive stress demand, severe neck pain and/or lower back pain might develop. Thus, frequent stretching and relaxing of muscles help reduce MSK pain.24 Similar findings have been obtained by Auerbach et al., reporting that lower back and neck pain were the most common pain among orthopaedic surgeons.6 In addition, Davis et al illustrated that lower back, neck, and shoulder pain are common among orthopaedic residents.7 Although these studies were conducted in different countries,6,7 they had similar results. This might lead to the conclusion that orthopaedic surgeons might experience lower back pain and neck problems due to excessive hours in the operating room, which also demands mechanical power. Besides, the use of surgical instruments and repetitive hand movements can contribute to the development of upper limb pain including elbow and wrist problems such as carpal or cubital tunnel syndrome.25
Moreover, there is a proportional rise in the incidence of knee pain and foot/ankle pain among participants with higher BMI. As surgeons are required to stand for long hours in the operation room, the excess weight might further exert pressure on the lower limb. Increase in body mass is associated with poorer locomotion and postural stability, which place the physician at risk of falling or being injured. A significant positive correlation was found between BMI and development of foot pain and disabilities, which may be due to both mechanical and metabolic mechanisms.26 Another systematic review indicated a clear correlation between increased BMI and unspecified foot pain.27 Previous studies illustrated an association between marital status and development of the work-related MSK pain as the one by Al-Mohrej et al.1 However, in the present study, no clear association was found between marital status and MSK pain which finding was consistent with Dianat et al.28 Therefore, socio-demographic factors should be taken into consideration in addition to psychological factors in future analysis of work-related MSK pain.
In our sample, orthopaedic surgeons who smoke were susceptible to lower back and hip/thigh pain compared with nonsmokers. This may be due to the deleterious effects of nicotine and hazardous chemicals found in cigarette smoke.29 Moreover, reduced oxygenation to the muscles might contribute to exacerbation of MSK pain.29 According to Zvolensky et al, individuals with a stable smoking history experience chronic back pain.29 In addition, experimental studies suggest organic pathogenesis involving toxic effects on osteoblasts/osteoclasts and hormonal changes.30 Thus, the provided information suggests a possible relationship between smoking habits and MSK complications.
The present study has shown an association between the lack of exercise and MSK pain development. Participants who are highly engaged in sports and are continuously active (51.4%) have reported fewer pain incidences compared to those who never exercise (48.6%). Exercising has improved neck, hip/thigh, and knee pain. Introduction of physical sports into daily routine might enable the physician to break through any dangerous habit and produce effective lifestyle changes. Eventually, with time, continuous stretching and strength training might reduce MSK-related pain. Similar results are obtained from a systematic review that illustrated the incorporation of strength exercises in MSK pain improvement.31 Strength exercises three times per week for at least 20 min contributes to successful pain management.31 According to Bernard et al, lifestyle changes, such as exercise, promote work breaks and behavioral changes which encourage the overall health during work hours.32
Moreover, orthopaedic surgeons with more than six years of clinical experience are more prone to shoulder/elbow, lower back, and hip/thigh pain compared to their youngster counterparts. However, years of experience have no role on pain development when adjusting for age. Age is a confounding factor in determining the incidence of lower back, hip/thigh, and knee pain. According to the data obtained, increasing age is correlated with worsening of MSK pain. This might be attributed to several factors including the weakening of muscles, deteriorating health, and accumulated muscular damage. This is speculated to be a result of accumulated musculoskeletal stress that led to various complaints. Tinubu et al stated that the increased number of clinical experience contributes to more MSK-related injuries and pain which supports our finding.33 Moreover, nurses who worked for 20 years are four-times more at risk of developing problems compared to less experienced nurses.33 They found that working in the same positions for long periods and treating high number of patients in one day were the main risk factors that participated in developing MSK-related injuries during the clinical experience.33 This was contradicted by Cromie et al, who revealed that youngsters are more vigorous at work and less oriented as compared with older professionals, leading to their susceptibility of developing MSK pain.34
Moreover, surgeons who excessively bend or twist for better access during their practice (84.4%) share a similar complaint of developing neck pain. This is attributable to the fact that surgeons remain in a particular position during operation. As surgeons continually look down, the neck muscles are facing severe demand and stress.
The effect of MSK pain on work was low, since only about 12% of the respondents took medical leave during the last 12 months due to work-related MSK pain. Compared to nurses who experienced back pain and sought medical care (58.7%),35 only around 30% of orthopaedic surgeons sought medical care for pain.
The limitations of our study include its cross-sectional design, which might limit the generalizability of the findings to larger populations. It is survey-based; thus, errors in recall may affect the reliability. Also, although online and email surveys allow respondents to maintain their anonymity, sending the survey via emails has its own disadvantages such as such as survey fraud, limited sampling, respondent and interviewer availability. Moreover, a major drawback is also that questionnaires were not received anonymously but by e-mail. In addition, subjective differences in the understanding of pain episodes or excessive bending cannot be ignored. As well, one of the major drawbacks was uncertain qualitative pain assessment. The study focused on certain predictors of MSK pain; however, psychological risk factors might also play a role. Because of the deficiency of prior data concerning the associations, our study’s multiple testing might lead to spurious associations that need further evidence. Therefore, our study aims to bring awareness and encourage further research about the topic. Further analysis with improved methodologies could be done to overcome these limitations. Also, further investigation is required to properly assess the issue and perhaps identify the risk factors that may participate in its development.
The study had not considered the foreign workforce which consists of 187 surgeons. However, this could be explained by the complexity and singularity of the Saudi health system. In Saudi Arabia, the vast majority of foreign orthopaedic workforce do not have the required privileges to do surgeries and procedures. So, they work in primary healthcare polyclinics where they refer the cases to higher centers. These centres, on the other hand, are occupied by Saudi surgeons. In addition to that, foreign orthopaedic workforces are rarely staying in the same position and in the same working environment for a long period of time since their positions are taken by the national people once they apply for the same job and carry similar qualifications. Due to the above-mentioned facts, the study group preferred not to include them as they are not considered a representative of a constant and steady working forces in the Saudi health system. As well, orthopaedic surgery remains the primary surgical speciality with the lowest proportion of female residents.36 This is also applicable in Saudi Arabia since the overall orthopaedic community intuitively dominated by men. As per Alshammari et al,37 62.0% of the female physicians in the Gulf Cooperation Council (GCC) found it difficult to be accepted in the orthopaedic programmes. At the time of the study in Riyadh, the number of Saudi females who work as orthopaedic surgeons was only nine. Of those, six were participants in our study (66.6%). Yet, statistical power is not accurate due to the small number of female participants.
Nonetheless, to further analyze and interpret the MSK pain among orthopaedic surgeons, proper prospective studies should be carried out. Future studies should aim to reveal the physical and psychosocial predictors of pain initiation. Although self-reported surveys may introduce some bias, they remain the most inexpensive and easily accessible method of collecting data. Physical examinations and long-term follow-up can be carried out as a more reliable source; however, they are very time-consuming and expensive. Furthermore, the analysis and explanation of published findings should be carefully done as many definitions are available for MSK conditions and several contributory factors may exist. Although limited data are available on the MSK pain among Saudi orthopaedic surgeons, this study mainly explored the prevalence of MSK-related problems among orthopaedic surgeons. Work stress and high physical demand along with lack of proper ergonomics might contribute to worsening of body pain. This will eventually, negatively influence the work environment and daily tasks. Awareness campaigns directed at orthopaedic surgeons to optimize their working environment might limit the negative effect of MSK pain on their productivity.
References
1. Al-Mohrej OA , AlShaalan NS , Al-Bani WM , Masuadi EM , Almodaimegh HS . Prevalence of musculoskeletal pain of the neck, upper extremities and lower back among dental practitioners working in Riyadh, Saudi Arabia: a cross-sectional study . BMJ Open . 2016 ; 6 ( 6 ): e011100 Crossref PubMed Google Scholar
2. Epstein S , Sparer EH , Tran BN , et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: A systematic review and meta-analysis . JAMA Surg . 2018 ; 153 ( 2 ): e174947 Crossref PubMed Google Scholar
3. Mirbod SM , Yoshida H , Miyamoto K , et al. Subjective complaints in orthopedists and general surgeons . Int Arch Occup Environ Health . 1995 ; 67 ( 3 ): 179 – 186 Crossref PubMed Google Scholar
4. Sargent MC , Sotile W , Sotile MO , Rubash H , Barrack RL . Quality of life during orthopaedic training and academic practice: part 2: spouses and significant others . J Bone Jt Surg Am . 2012 ; 94-A ( 19 ): e1451 – 1456 Crossref PubMed Google Scholar
5. Lester JD , Hsu S , Ahmad CS . Occupational hazards facing orthopedic surgeons . Am J Orthop (Belle Mead NJ) . 2012 ; 41 ( 3 ): 132 – 139 . PubMed Google Scholar
6. Auerbach JD , Weidner ZD , Milby AH , Diab M , Lonner BS . Musculoskeletal disorders among spine surgeons: results of a survey of the Scoliosis Research Society membership . Spine (Phila Pa 1976) . 2011 ; 36 ( 26 ): E1715 – 1721 Crossref PubMed Google Scholar
7. Davis WT , Sathiyakumar V , Jahangir AA , Obremskey WT , Sethi MK . Occupational injury among orthopaedic surgeons . J Bone Joint Surg Am . 2013 ; 95 ( 15 ): e107. https://doi.org/10.2106/JBJS.L.01427 Crossref PubMed Google Scholar
8. Alzahrani MM , Alqahtani SM , Tanzer M , Hamdy RC . Musculoskeletal disorders among orthopedic pediatric surgeons: an overlooked entity . J Child Orthop . 2016 ; 10 ( 5 ): 461 – 466 Crossref PubMed Google Scholar
9. Alqahtani SM , Alzahrani MM , Tanzer M . Adult reconstructive surgery: a high-risk profession for work-related injuries . J Arthroplasty . 2016 ; 31 ( 6 ): 1194 – 1198 Crossref PubMed Google Scholar
10. AlQahtani SM , Alzahrani MM , Harvey EJ . Prevalence of musculoskeletal disorders among orthopedic trauma surgeons: an Ota survey . Can J Surg . 2016 ; 59 ( 1 ): 42 – 47 Crossref PubMed Google Scholar
11. Attar SM . Frequency and risk factors of musculoskeletal pain in nurses at a tertiary centre in Jeddah, Saudi Arabia: a cross sectional study . BMC Res Notes . 2014 ; 7 ( 1 ): 61 Crossref PubMed Google Scholar
12. Keriri HM . Prevalence and risk factors of low back pain among nurses in operating rooms, Taif, Saudi Arabia . J Med Sci Res Journal of Medical Sceince & Research . 2013 ; 4 ( 1 ): 3 Google Scholar
13. Al-Eisa E , Al-Abbad H . Occupational back pain among rehabilitation nurses in Saudi Arabia: the influence of knowledge and awareness . Workplace Health Saf . 2013 ; 61 ( 9 ): 401 – 407 Crossref PubMed Google Scholar
14. Al-Mohrej OA , Mahabbat NA , Khesheaim AF , Hamdi NB . Characteristics and outcomes of obstetric brachial plexus palsy in a single Saudi center: an experience of ten years . Int Orthop . 2018 ; 42 ( 9 ): 2181 – 2188 Crossref PubMed Google Scholar
15. Kuorinka I , Jonsson B , Kilbom A , et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms . Appl Ergon England . 1987 ; 18 ( 3 ): 233 – 237 Crossref PubMed Google Scholar
16. Hirschfeld G , Zernikow B . Variability of ‘optimal’ cut points for mild, moderate, and severe pain: Neglected problems when comparing groups . Pain . 2013 ; 154 ( 1 ): 154 – 159 Google Scholar
17. Knudsen ML , Ludewig PM , Braman JP . Musculoskeletal pain in resident orthopaedic surgeons: results of a novel survey . Iowa Orthop J . 2014 ; 34 : 190 – 196 . PubMed Google Scholar
18. Wong T , Teo N , Kyaw M . Prevalence and risk factors associated with low back pain among health care providers in a district hospital . Malaysian Orthop J . 2010 . Google Scholar
19. AlQahtani SM , Alzahrani MM , Harvey EJ . Prevalence of musculoskeletal disorders among orthopedic trauma surgeons: An OTA survey . Can J Surg . 2016 ; 59 ( 1 ): 42 – 47 Crossref PubMed Google Scholar
20. Yasobant S , Rajkumar P . Work-Related musculoskeletal disorders among health care professionals: a cross-sectional assessment of risk factors in a tertiary Hospital, India . Indian J Occup Environ Med . 2014 ; 18 ( 2 ): 75 Crossref PubMed Google Scholar
21. Al-Arfaj AS , Alballa SR , Al-Dalaan AN , et al. Musculoskeletal pain in the community . Saudi Med J Saudi Arabia . 2003 ; 24 ( 8 ): 863 – 867 . Google Scholar
22. Moussa S , Al ZF , Alomar A , et al. Musculoskeletal pain in hail community: medical and epidemiology study; Saudi Arabia . Int J Sci Res . 2015 ; 4 ( 11 ): 1292 – 1299 . Google Scholar
23. Alghadir A , Anwer S . Prevalence of musculoskeletal pain in construction workers in Saudi Arabia . ScientificWorldJournal . 2015 ; 2015 ( 2 ): 1 – 5 Crossref PubMed Google Scholar
24. da Costa BR , Vieira ER . Stretching to reduce work-related musculoskeletal disorders: a systematic review . J Rehabil Med . 2008 ; 40 ( 5 ): 321-8 – 32328 Crossref PubMed Google Scholar
25. Barr AE , Barbe MF , Clark BD . Work-Related musculoskeletal disorders of the hand and wrist: epidemiology, pathophysiology, and sensorimotor changes . J Orthop Sports Phys Ther . 2004 ; 34 ( 10 ): 610 – 627 Crossref PubMed Google Scholar
26. Tanamas SK , Wluka AE , Berry P , et al. Relationship between obesity and foot pain and its association with fat mass, fat distribution, and muscle mass . Arthritis Care Res . 2012 ; 64 ( 2 ): 262 – 268 Crossref PubMed Google Scholar
27. Butterworth PA , Landorf KB , Smith SE , Menz HB . The association between body mass index and musculoskeletal foot disorders: A systematic review . Obes Rev . 2012 ; 13 ( 7 ): 630 – 642 Crossref PubMed Google Scholar
28. Dianat I , Bazazan A , Souraki Azad MA , Salimi SS . Work-Related physical, psychosocial and individual factors associated with musculoskeletal symptoms among surgeons: implications for ergonomic interventions . Appl Ergon . 2018 ; 67 : 115 – 124 Crossref PubMed Google Scholar
29. Zvolensky MJ , McMillan KA , Gonzalez A , Asmundson GJG . Chronic musculoskeletal pain and cigarette smoking among a representative sample of Canadian adolescents and adults . Addict Behav . 2010 ; 35 ( 11 ): 1008 – 1012 Crossref PubMed Google Scholar
30. Abate M , Vanni D , Pantalone A , Salini V . Cigarette smoking and musculoskeletal disorders . Muscles Ligaments Tendons J . 2013 ; 3 ( 2 ): 63 – 69 Crossref PubMed Google Scholar
31. Rodrigues EV , Gomes ARS , Tanhoffer AIP , Leite N . Effects of exercise on pain of musculoskeletal disorders: a systematic review . Acta ortop. Bras . 2014 ; 22 ( 6 ): 334 – 338 Crossref PubMed Google Scholar
32. Andersen CH , Andersen LL , Gram B , et al. Influence of frequency and duration of strength training for effective management of neck and shoulder pain: a randomised controlled trial . Br J Sports Med . 2012 ; 46 ( 14 ): 1004 – 1010 Crossref PubMed Google Scholar
33. Tinubu BM , Mbada CE , Oyeyemi AL , Fabunmi AA . Work-Related musculoskeletal disorders among nurses in Ibadan, south-west Nigeria: a cross-sectional survey . BMC Musculoskelet Disord . 2010 ; 11 : 12 Crossref PubMed Google Scholar
34. Cromie JE , Robertson VJ , Best MO . Work-Related musculoskeletal disorders in physical therapists: prevalence, severity, risks, and responses . Phys Ther . 2000 ; 80 ( 4 ): 336 – 351 Crossref PubMed Google Scholar
35. Abolfotouh SM , Mahmoud K , Faraj K , et al. Prevalence, consequences and predictors of low back pain among nurses in a tertiary care setting . Int Orthop . 2015 ; 39 ( 12 ): 2439 – 2449 Crossref PubMed Google Scholar
36. Chambers CC , Ihnow SB , Monroe EJ , Suleiman LI . Women in orthopaedic surgery: population trends in trainees and practicing surgeons . J Bone Joint Surg Am . 2018 ; 100 ( 17 ): e116 Crossref PubMed Google Scholar
37. Alshammari A , Shafiq M , Altayeb M , et al. Gulf cooperation Council female residents in orthopedics: influences, barriers, and mental pressures: a cross-sectional study . J Musculoskelet Surg Res . 2018 ; 2 ( 2 ): 51 Google Scholar
Author contributions
O. A. Al-Mohrej: Wrote the study proposal, collected the data, wrote, reviewed and approved the final manuscript.
A. K. Elshaer: Collected the data, wrote, reviewed and approved the final manuscript.
S. S. Al-Dakhil: Collected the data, wrote, reviewed and approved the final manuscript.
A. I. Sayed: Collected the data, reviewed and approved the final manuscript.
S. Aljohar: Did the statistical analysis, reviewed and approved the final manuscript.
A. A. AlFattani: Did the statistical analysis, reviewed and approved the final manuscript.
T. S. Alhussainan: Reviewed the study proposal, reviewed and approved the final manuscript.
OA. Al-Mohrej, AK. Elshaer and SS. Al-Dakhil contributed equally to this work.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Conflicts of interest
The authors declare that they have no competing interests.
Acknowledgements
Authors would to thank Ms. Lujain A. Bin Amer for her help in the data collection.
Ethical review statement
This study obtained the ethical approval from KFSH&RC Research advisory council (RAC#2191287).
Follow O. A. Al-Mohrej @MohrejO
Follow S. S. Al-Dakhil @saharaldakhil
Follow T. S. Alhussainan @Dr_Alhussainan
