




Abstract
Aims
The aim of this study was to evaluate the need for hand trauma services during the COVID-19 pandemic lockdown, specifically related to surgical requirements. This will provide useful information for planning and resource allocation in the event of any further lockdown.
Methods
A prospective analsysis of all patients attending our hand trauma unit throughout the UK COVID-19 lockdown period (24 March to 10 May 2020) was carried out. Prospectively collected departmental data from the same period in 2019 was obtained and reviewed for comparison. The number of patients attending clinic, undergoing surgery, the type of surgical procedure, and rate of surgery was compared.
Results
In all, 463 patients attended hand trauma services during the lockdown period compared to 793 in 2019 (32% reduction); 190 surgical procedures were carried out during lockdown compared to 236 in 2019 (20% reduction). Intervention rate was higher during the lockdown period (41% compared to 30%). There was no difference in the type of cases. In the first half of lockdown, 47% fewer procedures were performed than in 2019, but in the second half of lockdown 13% more procedures were carried out than the same period in 2019.
Conclusion
Requirements for hand trauma surgery remain high during a pandemic lockdown. Attendances and surgical requirements can be expected to steadily return to normal levels during a prolonged lockdown period. Throughout any future lockdown period adequate surgical provision must be maintained for patients with hand injuries.
Cite this article: Bone Joint Open 2020;1-10:639–643.
Take home message
Requirements for hand trauma surgery remain high during a pandemic lockdown.
Throughout any future lockdown period, adequate surgical provision must be maintained for patients with hand injuries.
Introduction
The World Health Organization (WHO) defined the coronavirus disease 2019 (COVID-19) outbreak as a pandemic on 11 March 2020. The first fatality in the UK was reported on 5 March 2020, and on 23 March the government announced a nationwide lockdown.1,2 This severely reduced movement for all UK citizens, with people allowed to leave their homes for essential purposes only, such as obtaining food or accessing healthcare. Only those with key workers jobs could continue their normal employment duties. This lockdown continued until 10 May, when restrictions were eased and a new alert scale system announced.
The COVID-19 pandemic has led to major, rapid reorganization of health services.3 Staff and resources were redeployed to deal with the huge surge in critically ill patients. This led to an almost complete cessation of elective services, and a large drop in patients seeking medical attention for emergency conditions.4,5 Despite this, hand trauma is expected to continue to occur during the pandemic. A significant proportion of hand injuries occur in the home or garden. Many key workers, including manual workers, continued in employment during the lockdown if they were supporting essential services. In our hand unit, we moved to a senior led seven day hand trauma service throughout the pandemic. The aim of this study was to evaluate the need for hand trauma services during the COVID-19 pandemic lockdown with particular regard to surgical requirements. This will provide useful information for planning and resource allocation in the event of any further lockdown, and for other countries yet to experience the pandemic.
Methods
Our large tertiary orthoplastic hand unit provides all hand trauma care to our local population of around 300,000 people. The unit also receives referrals from a large number of hospitals across the region and will accept tertiary referrals from anywhere across the UK. Many staff were redeployed during the lockdown period, but a senior core team of consultant hand surgeons, nurses and therapists was maintained. A seven-day trauma clinic was set up to see and treat any hand trauma patients who presented to the emergency department (ED). A small procedure room within the clinic was utilized to carry out procedures using local anaesthetic or wide awake local anaesthetic no tourniquet (WALANT) techniques.6
Prior to the pandemic, a daily trauma clinic took place five days a week (Monday to Friday) with access directly from the ED. A small amount of trauma cases were carried out in the procedure room, with the majority being listed on designated trauma lists during week days. At weekends, trauma patients would be referred to the on-call team, with most triaged and seen in a weekday clinic. Emergency cases would be reviewed in the ED, and urgent operating continued at the weekend using shared general emergency lists.
Immediately following the reorganization of our services, we initiated an audit of all trauma patients presenting to the trauma clinic. The study was reviewed and registered as an audit with the institutional audit group. Patient demographics, mechanism of injury, past medical history, length of inpatient stay, waiting time from clinic presentation to surgery, and treatment details were recorded. Procedures were grouped into seven categories: complex; fracture/dislocation; infection; ligament reconstruction; nail bed/fingertip; nerve/vessel repair; and wound/foreign body. A wound procedure denoted a non infected wound exploration with no significant structural injury. Infection procedures included drainage of abcesses, paronychia and washout and debridement of infected wounds. All patients who attended the clinic were included. Secondary checks were made of all procedure room and theatre lists to ensure all surgical data was obtained. The period studied was 24 March to 10 May 2020 inclusive. This 58-day period covers the whole of the main UK lockdown period.
Prospectively collected departmental routine data from the same period in 2019 was obtained and reviewed for comparison. The number of patients attending clinic, undergoing surgery, the type of surgical procedure and rate of surgery was compared. Comparison was also carried out between the first and second half of the lockdown period to identify if patient demographics and case type changed during this period.
A local polynomial regression smoothing function (locally estimated scatter plot smoothing) was fitted for the daily numbers of new trauma patients attending clinic and undergoing surgery for both study periods. Type of cases was compared using the chi squared goodness of fit test. Categorical data such as sex was analyzed using the Fisher’s exact test, parametric data with an unpaired t-test and non-parametric data with the Mann-Whitney U test. Normality of data was evaluated using the Kolmogorov-Smirnov test. Statistical analysis was performed with R.
Results
Overall, 463 patients attended the trauma clinic in the lockdown period compared to 793 in 2019 (32% reduction) (Table I). 190 surgical procedures were carried out compared to 236 in 2019 (20% reduction). Intervention rate was higher during the lockdown period (41% compared to 29.9%). There was no difference in the type of cases carried out between the two study periods. Sex was similar, but patients were significantly older in 2020. Length of inpatient stay was similar, but time to wait for surgery was shorter in 2020.
Table I.
Comparison of patient demographics and type of procedures performed during the 2020 lockdown and the corresponding period in 2019.
| Variable | 2019 | 2020 | p-value |
|---|---|---|---|
| Number | 236 | 190 | |
| Mean age, yrs (range) | 38.2 (2 to 82yrs) | 44.6 (9mths to 92yrs) | <0.001* |
| Sex M:F (male %) | 181:55 (77) | 151:39 (79) | 0.569† |
| All trauma patients, n | 793 | 463 | |
| Intervention rate, % | 30 | 41 | < 0.001† |
| Mean time to surgery, days (range) | 1.7 (0 to 8) | 0.2 (0 to 5) | < 0.001‡ |
| Mean length of stay, days (range) | 0.5 (0 to 10) | 0.2 (0 to 18) | 0.059‡ |
| Procedure, n (%) | 2019 | 2020 | |
| Complex | 8 (3) | 6 (3) | |
| Fingertip/nail bed | 41 (17) | 32 (17) | |
| Fracture/dislocation | 40 (17) | 25 (13) | |
| Infection | 27 (11) | 33 (17) | |
| Ligament recon | 3 (1) | 0 (0) | |
| Nerve/tendon repair | 48 (20) | 37 (20) | |
| Wound/foreign body | 69 (29) | 57 (30) | |
| p-value | N/A | 0.452§ |
-
*
Unpaired t-test.
-
†
Fisher’s exact test.
-
‡
Mann-Whitney U test.
-
§
Chi squared.
-
N/A, not applicable.
A noticeable increase in attendances and cases was seen in the second half of the lockdown period (Figure 1, Table II). Patient demographics and intervention rate were unchanged. Type of procedure was different in the second half of the lockdown period, with more fingertip injuries and nailbed repairs and infections, but the mechanism of injury remained similar.
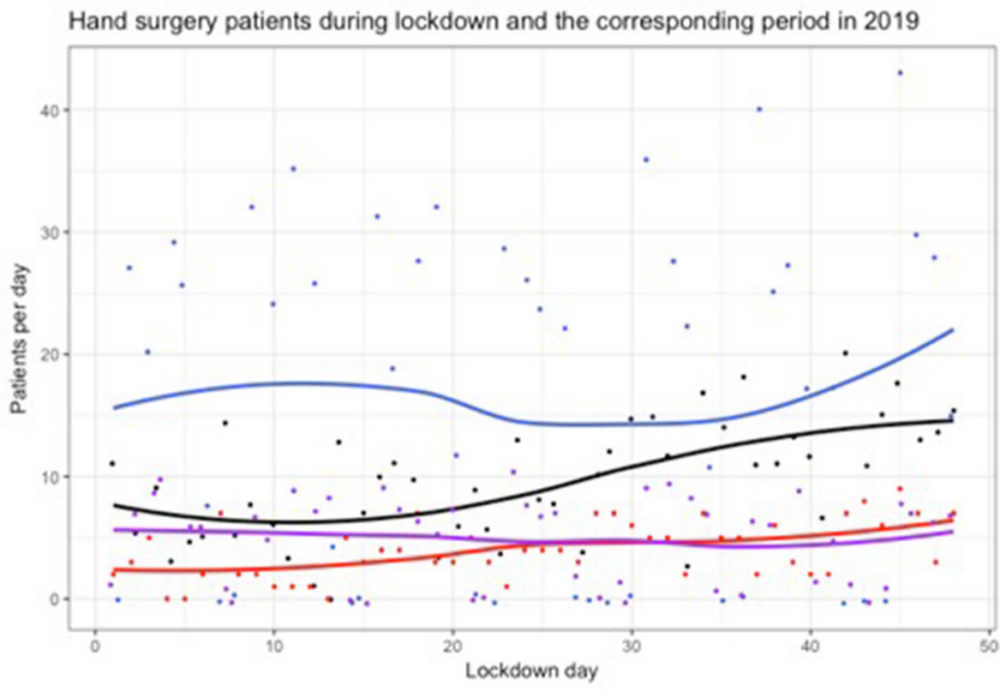
Fig. 1
Hand trauma activity during the COVID-19 lockdown and the corresponding period in 2019. Locally estimated scatterplot smoothing splines are fitted through the daily recorded counts, with datapoints, for clinic attendances (black) and cases (red) per day during lockdown and clinic attendances (blue) and cases (purple) per day in 2019.
Table II.
Comparison of patient demographics, type of procedures, and mechanism of injury of patients undergoing hand trauma surgery during the first and second halves of the 2020 lockdown.
| Variable | Days 1 to 24 | Days 25 to 48 | p-value |
|---|---|---|---|
| Number | 68 | 122 | |
| Mean age, yrs (range) | 44.4 (9 to 88) | 44.8 (9 months to 92 years) | 0.901* |
| Sex, M:F (male %) | 56:12 (82) | 95:27 (78) | 0.575† |
| Children, n (%) | 4 (6) | 11 (9) | 0.579† |
| All trauma patients, n | 167 | 296 | |
| Intervention rate, % | 41 | 41 | 0.922† |
| 2019, n | 128 | 108 | |
| Change from 2019, % | -47 | +13 | |
| Procedure, n (%) | |||
| Complex | 4 (6) | 2 (2) | |
| fFngertip/nail bed | 8 (12) | 24 (20) | |
| Fracture/dislocation | 11 (16) | 14 (12) | |
| Infection | 7 (10) | 26 (21) | |
| Nerve/tendon repair | 13 (19) | 24 (20) | |
| Wound/foreign body | 25 (37) | 32 (26) | |
| p-vaue | < 0.001‡ | ||
| Mechanism, n (%) | |||
| Animal bite | 1 (2) | 10 (8) | |
| Assault/punch | 5 (7) | 5 (4) | |
| Crush/trapped | 8 (12) | 17 (14) | |
| Fall | 5 (7) | 10 (8) | |
| Knife/tool | 34 (50) | 57 (47) | |
| No trauma/degenerative | 1 (2) | 3 (3) | |
| Spontaneous infection | 6 (9) | 11 (9) | |
| Sports | 5 (7) | 7 (6) | |
| Unknown | 3 (4%) | 2 (2%) | |
| p-value | 0.068‡ |
-
*
Unpaired t-test.
-
†
Fisher’s exact test.
-
‡
Chi squared.
Discussion
In this study, we have shown that requirements for hand trauma surgery remain high during a pandemic lockdown. Following a large decrease in hand trauma surgery cases at the start of the lockdown period, the number of cases steadily increased until they were higher than the number carried out the previous year. During the total lockdown period, the number of surgical procedures carried out only fell by 20% compared to the corresponding period in 2019. Case mix was remarkably similar. Total emergency new clinic attendances with hand trauma fell by 40%. The increase of cases needing surgical intervention, despite contemporaneous fears regarding surgical risk, suggest that either minor injuries did not present because of patient fears or did not happen. Evidence from presentation rates with serious medical illness suggests that there was a significant recalibration of patient expectations at that time.7,8
The COVID-19 pandemic quickly spread around the world, leading to major changes in healthcare delivery. An early international survey of hand surgeons demonstrated no agreement of best practise for hand surgery care.9 Several UK centres have subsequently published correspondence or short reports describing similar reorganization of services to those we used.10-12 See-and-treat principles, increased local anaesthetic and WALANT technique use, strategies to reduce follow-up visits, such as self removal of dressings and dissolvable sutures, along with virtual follow-up, have been widely used to provide safe and effective care for patients and staff during the pandemic.
New evidence regarding the COVID-19 pandemic and lockdown is constantly emerging. Several studies from the UK and across the world have shown a significant fall in musculoskeletal trauma attendances and surgical requirements.13-16 However, it has been demonstrated that incidence of some conditions, such as hip fractures, remains largely unaffected.16,17 Our study shows a high demand for surgical treatment of hand trauma is maintained. Attendances and surgical cases gradually increased during the lockdown following a large decrease at the start of the lockdown period. This is consistent with some gentle relaxation of the lockdown guidance and decreasing compliance from the public. More procedures were carried out for infection and fingertip/nail bed injuries during the second half of lockdown. Surgical intervention rate remained consistent. This was 10% higher than 2019 suggesting that more patients were presenting with significant injuries which required intervention. Patients were significantly older during the lockdown period. The reasons for this are unclear but may be due to less work place injuries which would occur in those of a working, younger age.
Garude et al18 reviewed patients admitted for hand trauma surgery during the first four weeks of the lockdown period, and compared this with the same period from 2019 in a large UK plastic surgery unit. Contrastingly, they reported a reduction of 56%. There was no difference in age and sex between the groups. These findings may reflect the early part of the lockdown which they studied. A survey of surgeons from Spain19 described a reduction in trauma attendances, although the majority felt the proportion of non-deferrable urgent procedures had not changed. Correspondence from a hand unit in Northern Italy reported no change in the number or type of hand trauma cases during the first month of their lockdown period.20 Hwee et al21 described no change in hand trauma workload during lockdown in Singapore. A letter from a plastic surgery unit in Dublin, Ireland, also reported no change in the number or type of hand trauma cases during the first 25 days of lockdown.22 The majority of these reports are consistent with our findings, and suggest that during COVID-19 lockdowns hand surgery need will remain significant across the world.
Injuries from tools and machinery most frequently affect the hand. Hampton et al23 carried out a multicentre retrospective review of trauma admissions during the first two weeks of lockdown and compared it with a similar period from 2019. The number of hand injuries was small, but they noted a significant increase in ‘do it yourself’ (DIY)-related hand injuries. Garude et al18 also noted a significant increase in the proportion of hand injuries associated with using tools at home. It seems that an expected reduction in work place injuries has had no effect on overall case numbers and more injuries are occurring at home and in the garden.
Limitations of the study include the retrospective analysis of the prospectively collected data from 2019. There was minimal data from this period regarding mechanism of injury, so comparison could not be carried out with 2020. Outcome data was not collected. Comparing outcome between the two periods was not the aim of this study but further research could investigate whether measures taken during the pandemic influenced patient outcome. We were unable to differentiate between work related and DIY injuries at home. We have compared actual numbers of patients and cases rather than rate. The population of the UK is estimated to be increasing by 0.6% each year so this is unlikely to have had a significant effect on the numbers seen.24 The 2019 data shows an obvious weekend effect in the regression graph with a dip seen due to the Easter bank holiday weekend (19 to 22 April 2019). This was not encountered during the Easter lockdown period due to the seven-day service. An equal number of bank holidays occurred during each year studied but there were two in the first half of the lockdown period with one in the second period. Holiday periods are known to effect trauma presentation but our data from the lockdown suggest this was not the case with our seven day service so this seems unlikely to influence our lockdown analysis findings. The loess regression smoothing method used will also account for small variations caused by factors such as this.
This study demonstrates that hand injuries continue to occur and require surgical treatment at a high rate during a pandemic lockdown. Attendances and surgical requirements can be expected to steadily return to normal levels during a prolonged lockdown period. Services in our unit were reconfigured to manage this trauma, but no elective work took place during this period. A large amount of hand trauma cases can be carried out using local anaesthetic or WALANT techniques. Throughout any future lockdown period, adequate provision must be maintained for patients with hand injuries and a significant amount of theatre capacity is required.
References
1. Department of Health and Social Care . 2020 . https://www.gov.uk/government/news/cmo-for-england-announces-first-death-of-patient-with-covid-19 (date last accessed 7 October 2020 ). Google Scholar
2. Office Prime Minister’s . Prime Minister’s statement on coronavirus (COVID-19) . 2020 . https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020 (date last accessed 7 October 2020 ). Google Scholar
3. World Health Organization (WHO) . Strengthening the health systems response to COVID-19: creating surge capacity for acute and intensive care . 2020 . https://www.euro.who.int/__data/assets/pdf_file/0006/437469/TG2-CreatingSurgeAcuteICUcapacity-eng.pdf?ua=1 (date last accessed 7 October 2020 ). Google Scholar
4. De Filippo O , D’Ascenzo F , Angelini F , et al. Reduced rate of hospital admissions for ACS during Covid-19 outbreak in northern Italy . N Engl J Med . 2020 ; 383 ( 1 ): 88 – 89 . Crossref PubMed Google Scholar
5. Thornton J . Covid-19: A&E visits in England fall by 25% in week after lockdown . British Medical Journal Publishing Group . 2020 : 369 – m1401 . Google Scholar
6. Lalonde D , Eaton C , Amadio P , Jupiter J . Wide-awake hand and wrist surgery: a new horizon in outpatient surgery . Instr Course Lect . 2015 ; 64 : 249 – 259 . PubMed Google Scholar
7. Mafham MM , Spata E , Goldacre R , et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England . Lancet . 2020 ; 396 ( 10248 ): 381 – 389 . Crossref PubMed Google Scholar
8. Sud A , Torr B , Jones ME , et al. Effect of delays in the 2-week-wait cancer referral pathway during the COVID-19 pandemic on cancer survival in the UK: a modelling study . Lancet Oncol . 2020 ; 21 ( 8 ): 1035 – 1044 . Crossref PubMed Google Scholar
9. Ducournau F , Arianni M , Awwad S , et al. COVID-19: initial experience of an international group of hand surgeons . Hand Surgery and Rehabilitation . 2020 . Crossref PubMed Google Scholar
10. Valand P , Lloyd N , Robson M , Steele J . Trauma transformed: a positive review of change during the COVID-19 pandemic . J Plast Reconstr Aesthet Surg . 2020 ; 73 ( 7 ): 1357 – 1404 . Crossref PubMed Google Scholar
11. Sadr MAH , Gardiner MS , Burr MN , Nikkhah MD , Jemec MB . Managing hand trauma during the COVID-19 pandemic using a one-stop clinic . J Plast Reconstr Aesthet Surg . 2020 ; 73 ( 7 ): 1357 – 1404 . Crossref PubMed Google Scholar
12. Venkatesan A , Iyengar K , Loh WYC . Strategies in reconfiguration of hand injuries management during COVID-19 pandemic . J Clin Orthop Trauma . 2020 ; 11 ( 4 ): 697 – 699 . Crossref PubMed Google Scholar
13. Christey G , Amey J , Campbell A , Smith A . Variation in volumes and characteristics of trauma patients admitted to a level one trauma centre during national level 4 lockdown for COVID-19 in New Zealand . N Z Med J . 2020 ; 133 ( 1513 ): 81 – 88 . PubMed Google Scholar
14. Morris D , Rogers M , Kissmer N , Du Preez A , Dufourq N . Impact of lockdown measures implemented during the Covid-19 pandemic on the burden of trauma presentations to a regional emergency department in Kwa-Zulu natal, South Africa . Afr J Emerg Med . 2020 : 10.1016/j.afjem.2020.06.005 . Crossref PubMed Google Scholar
15. Dayananda K , Yasin T , Jemmett P , Trickett R . Covid-19: the impact and changes to trauma services in Cardiff . Transient J Trauma, Orthopaed Coronavirus . 2020 ; 06 : 12 . Google Scholar
16. Murphy T , Akehurst H , Mutimer J . Impact of the 2020 COVID-19 pandemic on the workload of the orthopaedic service in a busy UK district general Hospital . Injury . 2020 ; 51 ( 10 ): 2142 – 2147 . Crossref PubMed Google Scholar
17. Scott CE , Holland G , Powell-Bowns MF , et al. Population mobility and adult orthopaedic trauma services during the COVID-19 pandemic: fragility fracture provision remains a priority . Bone Joint Open . 2020 ; 1 ( 6 ): 182 – 189 . Crossref PubMed Google Scholar
18. Garude K , Natalwala I , Hughes B , West C , Bhat W . Patterns of adult and paediatric hand trauma during the COVID-19 Lockdown . J Plast Reconstr Aesthet Surg . 2020 ; 73 ( 8 ): 1575 – 1592 . Crossref PubMed Google Scholar
19. Martin-Playa P , Calzacorta-Muñoz P , Aparicio Elizalde L , Carrera-Casal O , García Gutiérrez JJ . An overview of the situation of hand surgery in Spain during the peak of COVID-19 pandemic . Hand Surg Rehabil . 2020 ; 39 ( 5 ): 454 – 458 . Crossref PubMed Google Scholar
20. Facchin F , Messana F , Sonda R , Faccio D , Tiengo C , Bassetto F . COVID-19: initial experience of hand surgeons in northern Italy . Hand Surg Rehabil . 2020 ; 39 ( 4 ): 332 – 333 . Crossref PubMed Google Scholar
21. Hwee J , Chiew J , Sechachalam S . The impact of coronavirus disease 2019 (COVID-19) on the practice of hand surgery in Singapore . J Hand Surg Am . 2020 ; 45 ( 6 ): 536 – 541 . Crossref PubMed Google Scholar
22. Sugrue CM , Sullivan P . The effect of the ongoing COVID-19 nationwide lockdown on plastic surgery trauma caseload? J Plast Reconstr Aesthet Surg . 2020 ; 73 ( 7 ): 1357 – 1404 . Crossref PubMed Google Scholar
23. Hampton M , Clark M , Baxter I , et al. The effects of a UK lockdown on orthopaedic trauma admissions and surgical cases: a multicentre comparative study . Bone & Joint Open . 2020 ; 1 ( 5 ): 137 – 143 . Crossref PubMed Google Scholar
24. Office for National Statistics . Population estimates for the UK, England and Wales, Scotland and Northern Ireland: mid-2019 . 2019 . https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualmidyearpopulationestimates/latest (date last accessed 7 October 2020 ). Google Scholar
Acknowledgements
Thanks to Sarah Balmforth and Linda Tozer for helping with data collection and Laura Roberts for administrative assistance
Author contributions
F. Atia: Designed the study, Collected the data, Wrote and approved the manuscript.
S. Pocnetz: Collected and analyzed the data, Wrote and approved the manuscript.
A. Selby: Designed the study, Collected and analyzed the data, Wrote and approved the manuscript.
P. Russell: Designed the study, Wrote and approved the manuscript.
C. Bainbridge: Designed the study, Carried out analysis, Wrote and approved the manuscript.
N. Johnson: Designed the study, Collected and analyzed the data, Wrote and approved the manuscript.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
