




Abstract
Aims
COVID-19 remains the major focus of healthcare provision. Managing orthopaedic emergencies effectively, while at the same time protecting patients and staff, remains a challenge. We explore how the UK lockdown affected the rate, distribution, and type of orthopaedic emergency department (ED) presentations, using the same period in 2019 as reference. This article discusses considerations for the ED and trauma wards to help to maintain the safety of patients and healthcare providers with an emphasis on more remote geography.
Methods
The study was conducted from 23 March 2020 to 5 May 2020 during the full lockdown period (2020 group) and compared to the same time frame in 2019 (2019 group). Included are all patients who attended the ED at Raigmore Hospital during this period from both the local area and tertiary referral from throughout the UK Highlands. Data was collected and analyzed through the ED Information System (EDIS) as well as ward and theatre records.
Results
A total of 1,978 patients presented to the ED during the lockdown period, compared to 4,777 patients in the same timeframe in 2019; a reduction of 58.6%. Orthopaedic presentations in 2020 and 2019 were 736 (37.2%) and 1,729 (36.2%) respectively, representing a 57.4% reduction. During the lockdown, 43.6% of operations were major procedures (n = 48) and 56.4% were minor procedures (n = 62), representing a significant proportional shift.
Conclusion
During the COVID- 19 lockdown period there was a significant reduction in ED attendances and orthopaedic presentations compared to 2019. We also observed that there was a proportional increase in fractures in elderly patients and in minor injuries requiring surgery. These represented the majority of the orthopaedic workload during the lockdown period of 2020. Given this shift towards smaller surgical procedures, we suggest that access to a minor operating theatre in or close to ED would be desirable in the event of a second wave or future crisis.
Introduction
The Coronavirus disease 2019 (COVID-19) pandemic has been a new global experience for all aspects of society, including the healthcare system.1 It has affected and changed many rules, pathways, and systems which relate to orthopaedics.2 It remains the major focus of healthcare provision and provides a challenging background for the gradual resumption of previously routine work. Despite this crisis, trauma and orthopaedic presentations have not stopped. Consequently, the challenge is how to manage orthopaedic emergencies effectively, while at the same time protecting patients and staff from this disease.
This study was conducted at Raigmore Hospital, an acute district general teaching hospital located in the Highlands of Scotland. It serves a population of around 234,770 and covers an area approximately the size of Belgium. Tertiary services are available in the central belt of Scotland and Aberdeen which are a two- to three-hour drive from our hospital.3,4
Raigmore Hospital is the largest healthcare hub in our region, which is also served by three rural general hospitals (RGH) in the towns of Wick, Fort William, and Broadford on the Isle of Skye. Each of these ‘spoke’ hospitals is around two to three hours by road. Each of the RGHs has its own emergency department (ED) and is able to manage simple injuries and fractures with advice available from Raigmore. If surgery is required, however, the patients are transferred to Raigmore Hospital. Our geography is unique within the UK and the NHS but draws parallels with many of the more remote areas elsewhere in the world.4
The ongoing COVID-19 pandemic spread to the UK in late January 2020.5 As of 31 May 2020, there have been 274,762 confirmed cases and 38,489 confirmed deaths overall, the third-highest death rate in the world.6,7 The UK was put into an unprecedented national lockdown on 23 March. In early May, some restrictions were relaxed in England with a similar decision made in late May in Scotland.8,9
This study focuses on the period of complete lockdown, often referred to as “mass quarantine”, where residents were advised to stay at home. This involved restricting movement by only allowing people to leave home to attend essential work, acquire food or medicine, go to hospital or to exercise once a day.9 We explored how the lockdown affected the rate, distribution, and type of orthopaedic trauma ED presentations, using the same period in 2019 as reference. This article discusses considerations for the ED and trauma wards to help to maintain the safety of the patients and healthcare providers.
In May 2020, Hampton et al10 described their experiences of the lockdown on the orthopaedic service in a multicentre study performed over a period of two weeks either side of the government restrictions imposed. They saw a reduction in ED attendances by greater than 50%. The aim of this project is to apply a similar analysis, but over a period of time encompassing the entire period of restrictions. Our population is relatively unique within the UK as a result of our rural geography.
Methods
The study was conducted from 23 March 2020 to 5 May 2020 during the full lockdown period (2020 group) and compared to the same time frame in 2019 (2019 group). Included are all patients who attended the ED at Raigmore Hospital during this period from both the local area and tertiary referral from throughout the Highlands.
The ED cases were triaged at the front door into green and red categories in line with accepted pandemic practice. For the purpose of analysis of our data, we determined that ‘major injuries’ included polytrauma, fractures of lower limb long bones, hip fractures, spine, and pelvic fractures. Minor injuries included sprains, strain, limb minor fractures and soft tissue injuries, pain in a joint, localized limb infections, and joint dislocations. Our orthopaedic team attended to all minor injuries as well as the major orthopaedic cases. Head, face, chest, abdominal injuries, burns, bites, and foreign bodies were excluded.
Minor procedures included closed fracture or dislocation reduction, Kirshner wire insertion, wound washout/exploration, tendon repair, abscess drainage, or wound closure. They were predominantly performed under local anaesthetic, regional block, or sedation. Major procedures included open reduction and implant insertion, arthroplasty for hip fracture, and any procedure with significant anticipated blood loss. These were done under regional or general anaesthetic.
Admissions were classified as major or minor. ‘Minor’ admissions included patients who presented with a minor injury and were admitted for a minor procedure, observation or intravenous antibiotics. All other admissions were categorized as ‘major’.
Retrospective data of the study was collected and analyzed through the Emergency Department Information System (EDIS) as well as ward and theatre records. Patients with incomplete data were excluded.
Statistical analysis
Data was coded and entered using SPSS v. 26 (IBM, Armonk, New York, USA). Data was summarized using mean and SD for quantitative variables and frequencies (count) and relative frequencies (percentages) for categorical variables. Continuous variables were age, total number of cases, and mean number of presentations per day. Categorical variables were sex, type of injuries, fractures, and whether the patients required admission and/or surgery. Comparisons between groups was done using independent-samples t-tests.11 For comparing categorical data, chi-squared tests were performed. Fisher's Exact test was used instead when the expected frequency was less than five.12 A p-value less than 0.05 was considered statistically significant.
Results
A total of 1,978 patients presented to the ED during the period of 44 days during the lockdown, compared to 4,777 patients in the same period of 2019; a reduction of 58.6% (p < 0.001 independent-samples t-test). Orthopaedic presentations in 2020 and 2019 were 736 (37.2%) and 1729 (36.2%) respectively, representing a 57.4% reduction (Table I).
Table I.
Total number of cases presented to ED, mean number per day, total orthopaedic presentations and total fractures-dislocations in 2020 (lockdown) and 2019 groups.
| Variable | 2020 | 2019 | Reduction, % | p-value |
|---|---|---|---|---|
| Total attendances | 1,978 | 4,777 | 58.6 | |
| Mean cases per day, n (SD) | 15.18 (5.3) | 36.75 (9.7) | 58.7 | < 0.001* |
| Orthopaedic presentations, n (%) | 736 (37.2) | 1729 (36.2) | 57.4 | 0.430† |
| Fractures, n (%) | 262 (13.2) | 468 (9.8) | 44.0 | < 0.001† |
-
*
Independent-samples t-test.
-
†
Chi-squared test.
In the 2020 group, the mean age was 43.33 years (SD 25.02) and included 329 males (44.7%) and 407 females (55.3%). In 2019 group, the mean age was 39.48 years (SD 23.98) and included 934 males (54%) and 795 females (46%) (p < 0.001 chi-squared test; Table II). In 2019 there was a higher proportion of patients in their second and third decades whereas in 2020 a higher proportion of elderly patients was observed. Fractures in patients aged above 60 years was 105 (40%) vs 160 (34.2%) in 2019 (Figures 1 and 2).
Table II.
Age and sex distribution of the orthopaedic presenting patients in the two groups.
| Variable | 2020 (n = 736) | 2019 (n = 1,729) | p-value |
|---|---|---|---|
| Mean age, yrs (SD) | |||
| Orthopaedic presentations | 43.33 (25.02) | 39.48 (23.98) | < 0.001* |
| Fracture group | 48.17 (27.33) | 43.42 (27.32) | 0.024* |
| Sex, M: F (%) | 329:407 (44.7:55.3) | 934:795 (54:46) | < 0.001† |
-
*
Independent-samples t-test.
-
†
Chi-squared test.
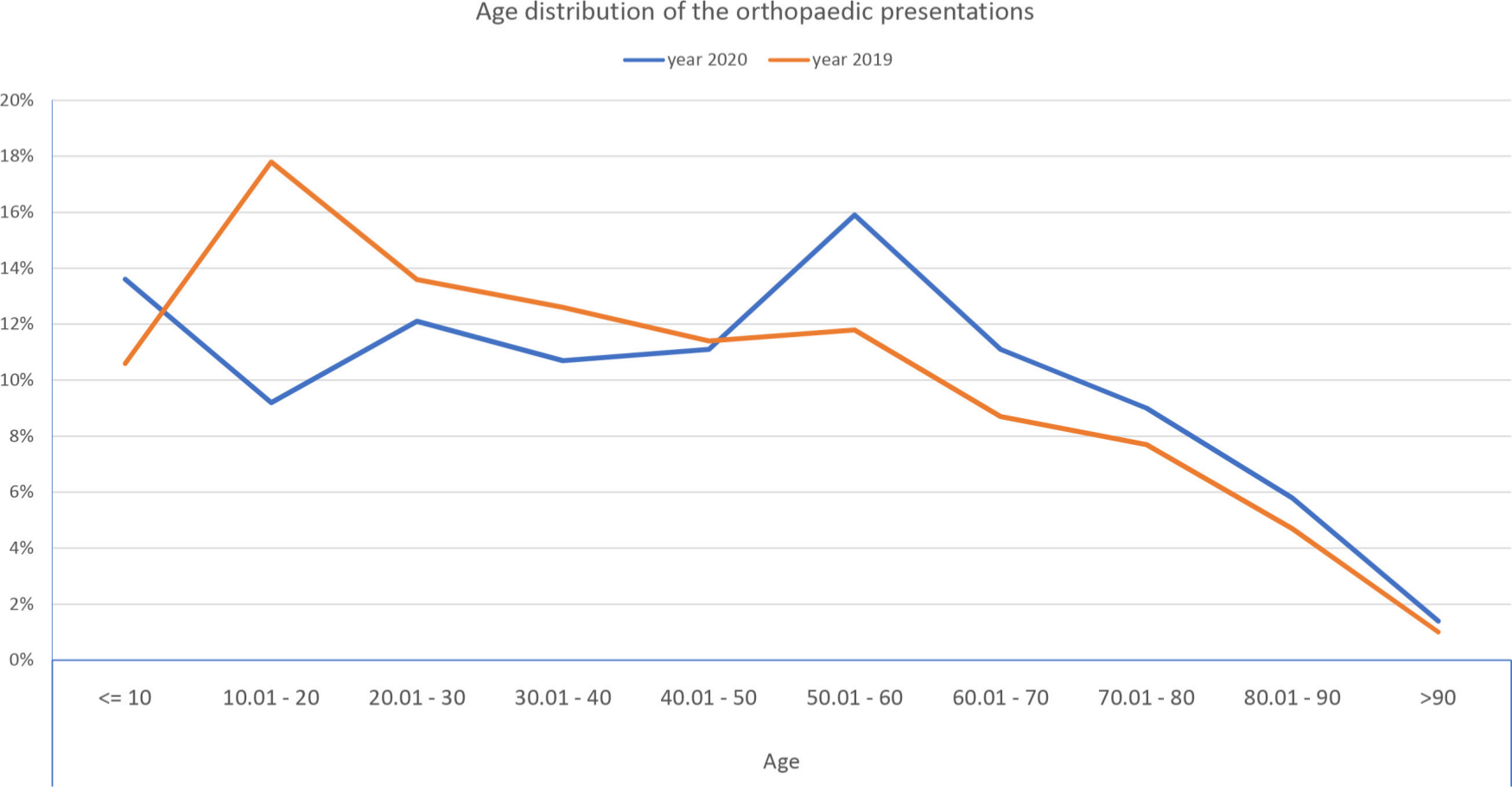
Fig. 1
Illustration of the age distribution of emergency department orthopaedic presentations.
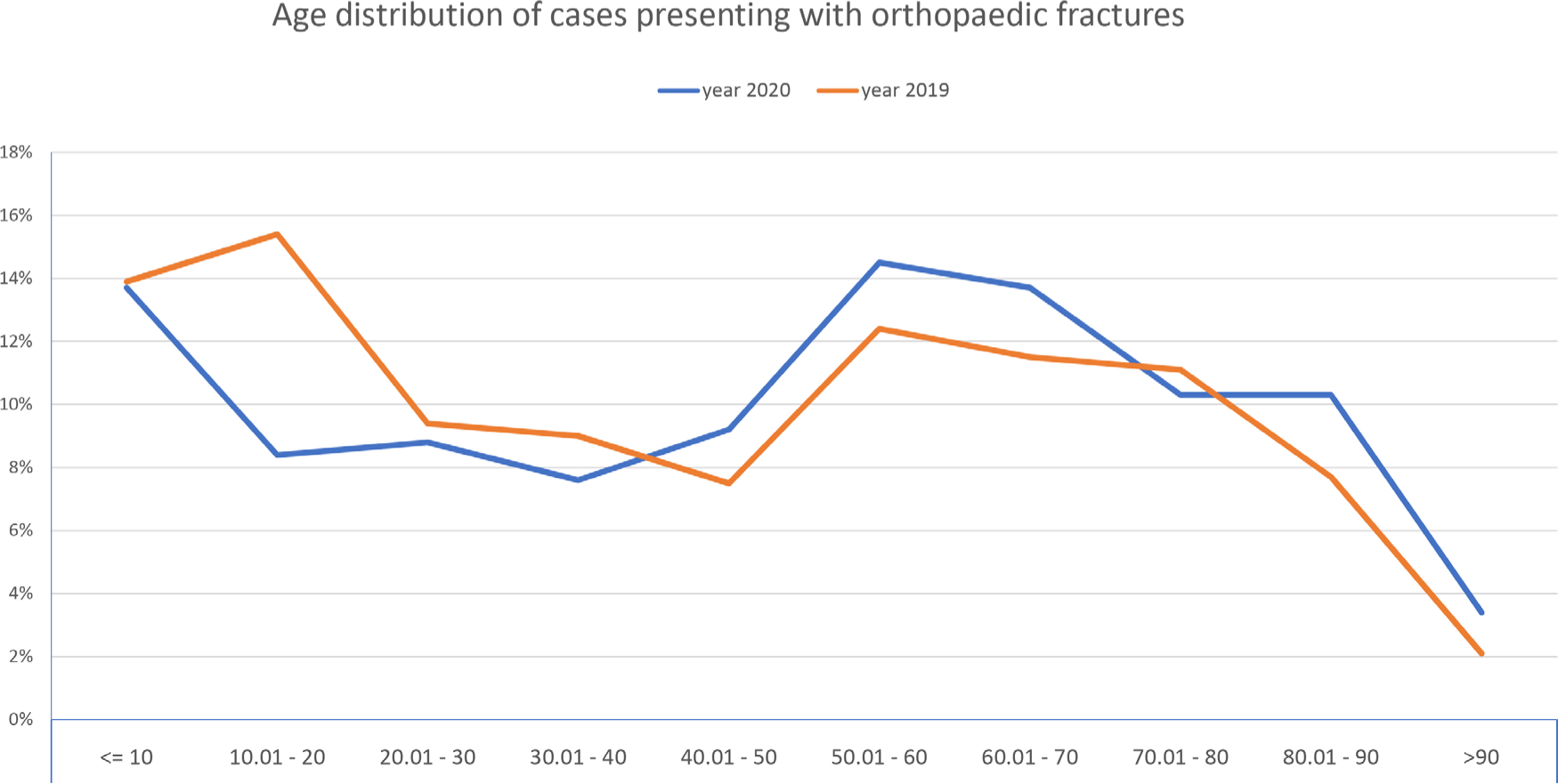
Fig. 2
Illustration of the age distribution of cases sustained orthopaedic fractures.
Minor presentations accounted for 514 patients (69.8%) of the total orthopaedic presentations in 2020 during the pandemic. Minor injuries include: sprains and contusions 249 (33.8%); abrasions and lacerations 119 (16.2%); joint pain 38 (5.2%); and and infections 25 (3.4%). There were 172 hand injuries (23.4%; Table III).
Table III.
Different types of emergency department presentations.
| Presentation, n (%) | 2020 (n = 736) | 2019 (n = 1,729) | p-value* |
|---|---|---|---|
| Hand injuries | 172 (23.4) | 364 (21) | 0.202 |
| Foot injuries | 55 (7.5) | 135 (7.8) | 0.775 |
| Sprains and soft tissue contusions | 249 (33.8) | 721 (46.5) | < 0.001 |
| Joint pain/arthritis/LBP | 38 (5.2) | 85 (4.9) | 0.797 |
| )Infections/tenosynovitis | 25 (3.4) | 94 (5.4) | 0.031 |
| Abrasions/lacerations | 119 (16.2) | 212 (13.6) | 0.009 |
| Total minor presentations | 514 (69.8) | 1349 (78) | < 0.001 |
| Total requiring admission (minor:major, %) |
133 (18) (57.2:42.8) | 249 (14.4) (39:61) | 0.021 |
| Total requiring admission and surgical intervention | 110 (14.9) | 210 (12.2) | 0.046 |
-
*
Chi-squared test.
-
LBP, lower back pain.
The total number of admissions to orthopaedic wards was 133 patients (18% of ED attendances) and 249 patients (14.4%) in 2020 and 2019, respectively (p = 0.021, chi-squared test). Of these, 110 and 210 of the admitted patients required surgical intervention in 2020 and 2019 groups respectively (Table III).
During the lockdown period, there were 262 patients (35.6% of the orthopaedics presentations, 13.2% of the total ED attendances) who had sustained a fracture or dislocation, representing a 44% reduction comparing to 2019 (p < 0.001, chi-squared test; Table I, Table IV, Figure 3). There was a reduction in polytrauma and open fracture cases during lockdown. Four patients (0.54%) sustained polytrauma versus 21 patients (1.2%) in 2019 and seven patients (2.6% of total orthopaedic fracture presentations) presented with open fracture versus 15 patients (3.2%) in 2019.
Table IV.
Comparison between types of the fractures and dislocations in the two groups.
| Type, n (%) | 2020 (n = 262) | 2019 (n = 468) |
|---|---|---|
| Hand/Foot | 62 (23.7) | 130 (27.8) |
| Wrist | 51 (19.5) | 88 (18.8) |
| Hip | 33 (12.6) | 43 (9.2) |
| Ankle | 31 (11.8) | 49 (10.5) |
| Humerus | 25 (9.5) | 26 (5.6) |
| Dislocations | 25 (9.5) | 54 (11.5) |
| Elbow | 12 (4.6) | 18 (3.8) |
| Clavicle | 11 (4.2) | 24 (5.1) |
| Spine | 2 (0.8) | 13 (2.8) |
| Others* | 10 (3.8) | 23 (4.9) |
-
*
Other fractures (pelvis, knee and other long bones).
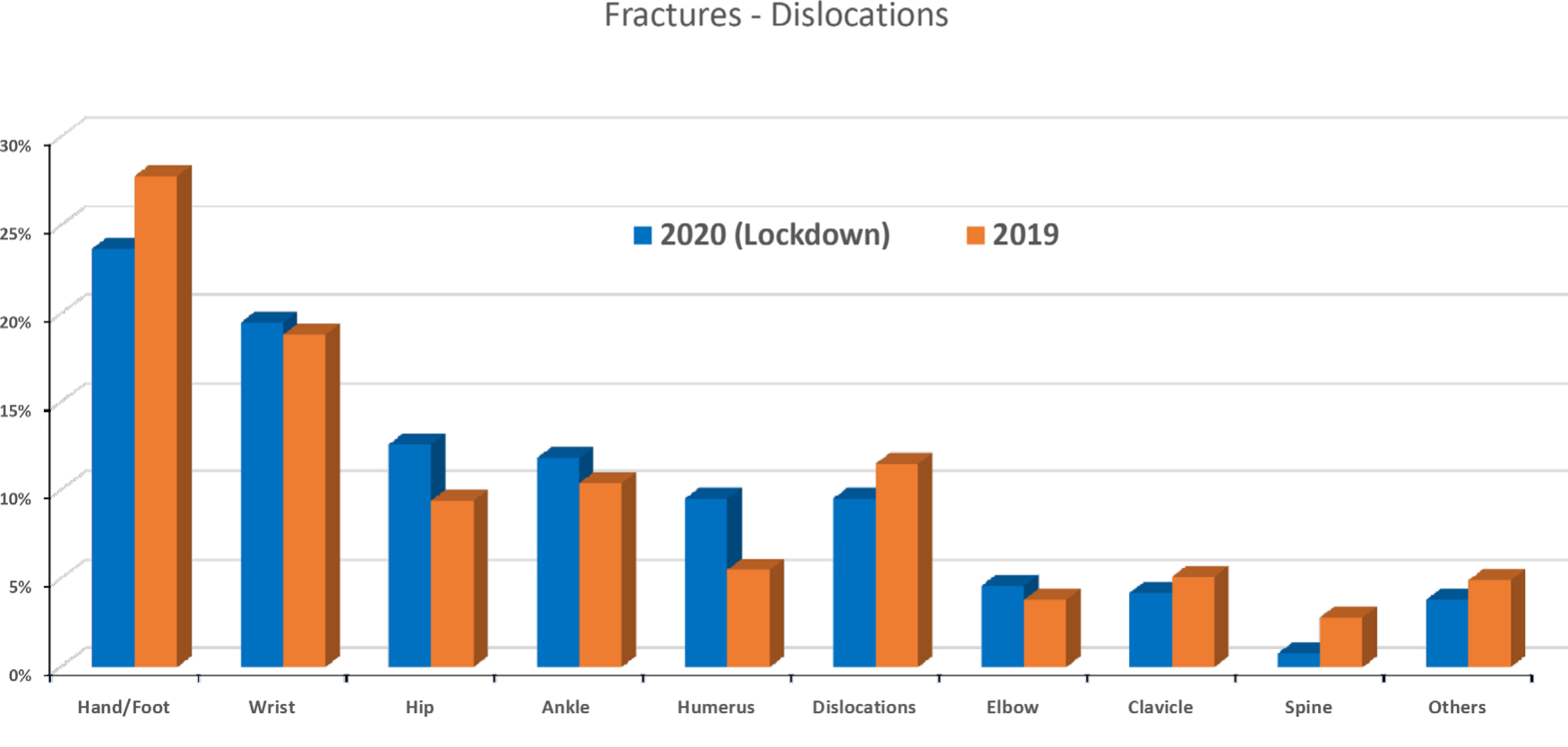
Fig. 3
Distribution of the different types of fractures during the pandemic lockdown period and 2019.
The total number of operated cases during the pandemic lockdown was 110, of which 48 (43.6%) were major procedures and 62 (56.4%) were minor procedures. During the same period of 2019, 210 cases were performed, of which 135 (64.3%) were major procedures and 75 (35.7%) were minor procedures (p < 0.001, Fisher's Exact test; Table V, Figure 4).
Table V.
Comparison of surgical cases in 2020 and 2019.
| Procedure, n (%) | 2020 | 2019 | p-value |
|---|---|---|---|
| Hip* | 33 (30) | 43 (16.2) | 0.004† |
| ORIF‡ | 15 (13.6) | 92 (43.8) | < 0.001† |
| Total major | 48 (43.6) | 135 (64.3) | < 0.001† |
| Total minor | 62 (56.4) | 75 (35.7) | < 0.001† |
| Total procedures | 110(14.9) | 210 (12.1) | 0.046§ |
-
*
Hip fractures managed by internal fixation or arthroplasty.
-
†
Fishers Exact test.
-
‡
Other than hip fractures.
-
§
Chi-squared test.
-
ORIF, open reduction internal fixation.
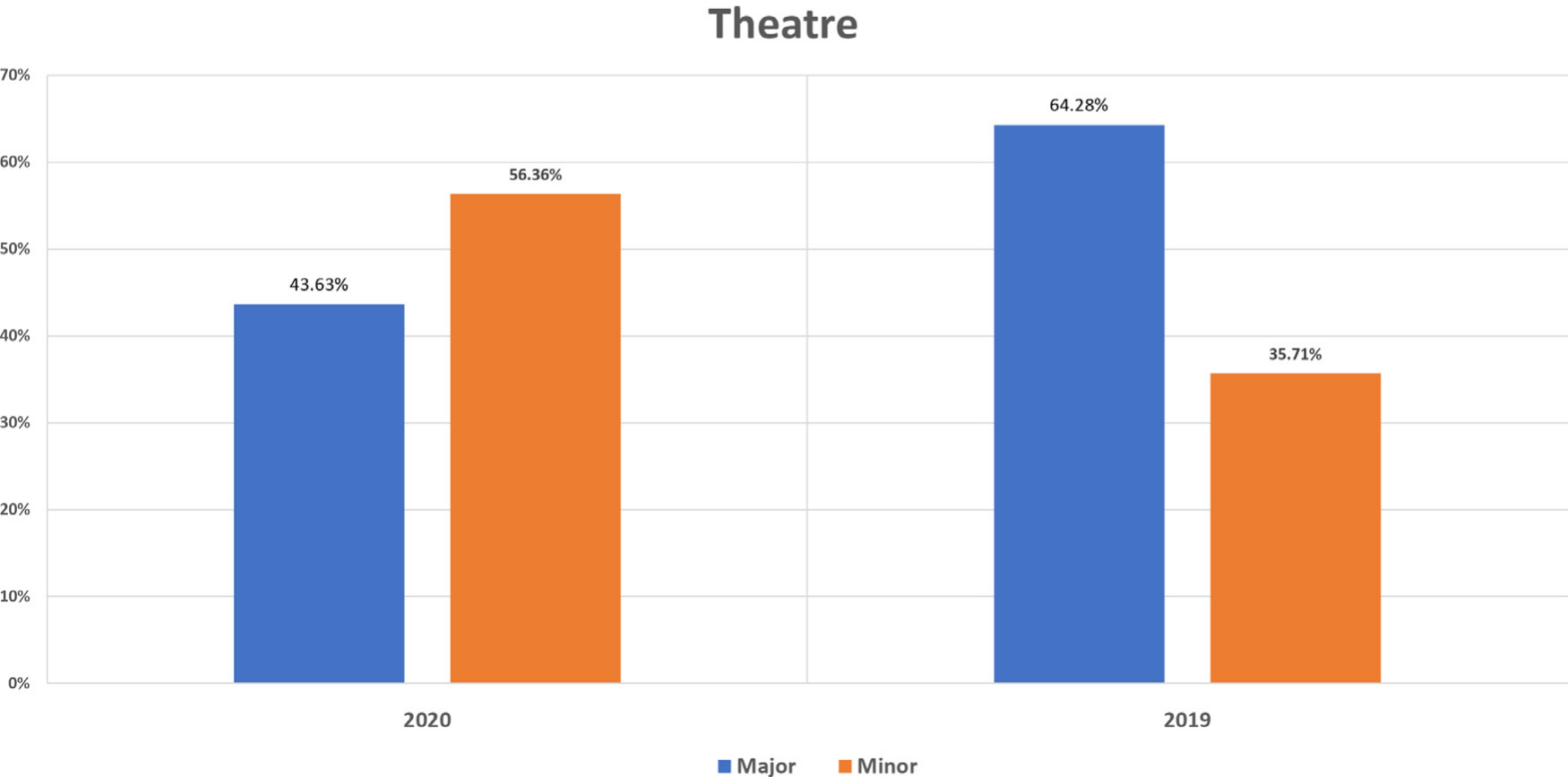
Fig. 4
Illustration of the theatre procedures in the two groups.
Discussion
The authors are keen to document their experience, in the knowledge that every new piece of evidence could improve systems during COVID-19 and provide a guide for orthopaedic teams in other hospitals. We observed a reduction in the total ED attendances of (58.6%) in lockdown compared to 2019 (1.978 in 2020 vs 4,777 in 2019). Orthopaedic presentations reduced by 57.4% and fracture/dislocation by 44% (736 in 2020 vs 1,729 in 2019 and 262 in 2020 vs 468 in 2019, respectively).
Minor injuries requiring minor surgery represented the majority of orthopaedic workload during the lockdown period of 2020. There was decrease in number and ratio of polytrauma and open fractures during the COVID 19 lockdown. This differs when compared to the same period in 2019. We suggest that this is as a result of reduced road traffic and reduced participation in outdoor pursuits such as mountaineering and cycling. There was a significant proportional increase in ED presentations for abrasions and lacerations and a proportional increase, albeit non-significant (p = 0.202, chi-squared test), of hand injuries in 2020 compared to 2019. We propose this is a result of an increase in home and garden improvement do-it-yourself (DIY) projects brought about by increased time spent at home.
We observed that the number of minor injuries presenting to ED during lockdown was significantly lower (p < 0.001, chi-squared test) but the proportion of those requiring admission or surgery was significantly higher (p < 0.001, chi-squared test). We propose two reasons for this. Firstly, the number of patients presenting with sprains and contusions was far higher in 2019. This type of injury is often sustained during physical activity such as contact sports and outdoor pursuits which were not taking place during the lockdown period. Secondly, patients with this type of injury would in our view be less likely to present due to fear of contracting COVID-19.
In patients who sustained fractures, fragility and low velocity fractures predominated. Specifically, the proportion of wrist, hip, and humeral fractures was higher during 2020 than 2019.
There was a higher proportion of fractures in elderly patients during the lockdown of 2020 compared to 2019. This is most likely due to their pre-existing risk of fragility fracture from low energy trauma.13 The reduction in the proportion of non-fragility fractures can be explained by fewer people undertaking activities which can cause injury, including cycling, climbing, and industrial work. In addition, the restrictions imposed on travel will have led to a significant reduction on tourist travel during the start of the busy holiday season in the Scottish Highlands.
The British Orthopaedic Association (BOA) issued guidelines in April 2020 as the pandemic was in its early stages in the UK.14 These guidelines suggested an emphasis towards a more conservative approach to many trauma cases and as a result there are likely to have been fractures which were managed non-surgically which may previously have undergone more aggressive intervention.15 This could explain further the reduction of major procedures in lockdown vs 2019 (48 (43.6%) vs 135 (64.3%)).
During the COVID-19 pandemic period of spring 2020, our orthopaedic department underwent significant reconfiguration. Due to the increasing demands placed upon their workforce, the ED minors department was staffed almost exclusively by members of the orthopaedic team between 9 am and 9 pm. This allowed rapid throughput of minor trauma patients with a senior orthopaedic decision maker present seven days a week during this period.15
A sizeable proportion of our workload is generated from our peripheral rural general hospitals. We adopted the same approach to these patients as with local patients, only those requiring surgery were transferred to Raigmore hospital. Our pre-existing model of virtual fracture care proved invaluable during this period.
As recommended by the BOA guidelines, a second on call or lead consultant was appointed for each 24 hour period and there was a separate trauma operating team each day. An emphasis was placed upon early and accurate patient information delivered face to face and in writing to promote self-management. A daily virtual fracture clinic performed by one or more consultants provided a safety net for inappropriately managed injuries.14 We are not aware at time of writing of any injuries deemed to have been missed or managed inappropriately. Maintaining consistent, regular, and accurate communication is vital and daily briefs by the orthopaedic and ED departments were conducted seven days a week.
Reflecting upon our experience over the pandemic period, and given the likelihood of further similar pandemic periods increases,16 we considered the following changes to delivery of orthopaedic care moving forward. The unprecedented situation of the COVID-19 pandemic has highlighted the need for advancements in the use of technology to minimize hospital footfall to only those who need to be there. Using digital patient communication platforms such as NHS Near Me17 and senior decision making before the first face to face contact may reduce hospital attendances. The rural location of our service and consequently our prior familiarity with these technologies and procedures meant that many of these processes were already in place and adjustment was straightforward.
If staffing levels and the hospital capacity permit, it would be desirable to have separate ‘green’ and ‘red’ teams in both major and minor injuries units, having demonstrated that minor injuries represent the majority of orthopaedic admissions and procedures during a pandemic lockdown period. Having a temporary minor operating theatre in our unit, ideally adjacent to ED, would have markedly reduced the number of hospital admissions and potential viral exposure to patients. As such, this would be desirable in the future to permit minor surgical procedures such as wound care, fracture/joint manipulation and simple instrumentation (e.g. Kirschner wiring).
Addition of a mini C-arm and capability of delivering local, regional anaesthesia or sedation, avoiding the aerosol generating general anaesthesia risk, would also be desirable. This could be delivered with the help of the anaesthetic team or through specific training of the orthopaedic team in these skills. Ideally, this theatre would be connected to a recovery-discharge room.
Our figures suggest that up to 56% of our surgical workload could have been performed if there was access to a minor operating theatre adjacent to the ED minors department. This would reduce the burden on ward staff and free up beds for more urgent cases. Although there was no discernible change in threshold for offering operative intervention, the principle of thorough consideration of non-surgical treatment was certainly emphasized during this period.18
Despite being a local and tertiary referral hospital, we operate in a relatively unique environment of large area with relatively small population. A larger sample size and multicentre study may more accurately reflect effect of lockdown in UK as a whole. Further investigations, planning, and design will be needed for each centre to have a ready standby minor operative room which can be opened, should a second wave or any future similar crisis occur.
Although there was a dramatic reduction of ED attendances and orthopaedic presentations during the COVID- 19 lockdown period compared to 2019, we observed that there were changes in the age distribution of the orthopaedic presentations and the fractures occurred predominantly in the more elderly fragility fracture population during the lockdown. We also observed that a greater proportion of admissions and theatre cases were as a result of minor injuries such as lacerations, many of which were sustained during stay-at-home activities such as DIY.
This paper has shown that minor injuries admissions and procedures represented a higher proportion of the orthopaedic work during the crisis compared with an equivalent non pandemic period. We therefore suggest that management of these injuries within the ED with increased surgical capability, as would be provided with a minor operating theatre could be a viable option to reduce the risks to both patients and staff.
References
1. World Health Organization (WHO) . Coronavirus disease 2019 (COVID-19) situation report – 52 . 2020 . https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200312-sitrep-52-covid-19.pdf?sfvrsn=e2bfc9c0_4 (date last accessed 8 April 2020 ). Google Scholar
2. Chang Liang Z , Wang W , Murphy D , Po Hui JH . Novel coronavirus and orthopaedic surgery: early experiences from Singapore . J Bone Joint Surg Am . 2020 ; 102-A ( 9 ): e000236 . Crossref PubMed Google Scholar
3. Mascarenhas M , Beattie M , Roxburgh M , et al. Using the model for improvement to implement the Critical-Care pain observation tool in an adult intensive care unit . BMJ Open Qual . 2018 ; 7 ( 4 ): e000304 . Crossref PubMed Google Scholar
4. NHS Highland . Raigmore Hospital . 2020 . https://www.nhshighland.scot.nhs.uk/ services/ pages/ raigmorehospital.aspx (date last accessed 9 June 2020 ). Google Scholar
5. Lillie PJ , Samson A , Li A , et al. Novel coronavirus disease (Covid-19): the first two patients in the UK with person to person transmission . J Infect . 2020 ; 80 ( 5 ): 578 – 606 . Crossref PubMed Google Scholar
6. GOV.UK Coronavirus (COVID-19) cases in the UK . UK crown coronavirus (COVID-19) in the UK . 2020 . https://coronavirus.data.gov.uk/ (date last accessed 31 May 2020 ). Google Scholar
7. Johns Hopkins Coronavirus Resource Center . Mortality in the most affected countries . 2020 . https://coronavirus.jhu.edu/map.html (date last accessed 31 May 2020 ). Google Scholar
8. National Records of Scotland . Deaths involving coronavirus (COVID-19) in Scotland . 2020 . https://www.nrscotland.gov.uk/ covid19stats (date last accessed 31 May 2020 ). Google Scholar
9. BBC News . PM announces strict new curbs on life in UK . 2020 . https://www.bbc.co.uk/news/uk-52012432 (date last accessed 10 May 2020 ). Google Scholar
10. Hampton M , Clark M , Baxter I , et al. The effects of a UK lockdown on orthopaedic trauma admissions and surgical cases . Bone & Joint Open . 2020 ; 1 ( 5 ): 137 – 143 . Crossref PubMed Google Scholar
11. Chan YH . Biostatistics 102: quantitative data--parametric & non-parametric tests . Singapore Med J . 2003a ; 44 ( 8 ): 391 – 396 . PubMed Google Scholar
12. Chan YH . Biostatistics 103: qualitative data - tests of independence . Singapore Med J . 2003b ; 44 ( 10 ): 498 – 503 . PubMed Google Scholar
13. NHS England . Clinical guide for the perioperative care of people with fragility fractures during the coronavirus pandemic . 2020 . https://www.england.nhs.uk/coronavirus/wpcontent/uploads/sites/52/2020/03/C0086_Specialty-guide-_Fragility-Fractures-and-Coronavirus-v1-26-March.pdf (date last accessed 10 April 2020 ). Google Scholar
14. British Orthopaedic Association . Emergency BOAST: management of patients with urgent orthopaedic conditions and trauma during the coronavirus pandemic . 2020 . https://www.boa.ac.uk/resources/covid-19-boasts-combined.html (date last accessed 15 May 2020 ). Google Scholar
15. NHS England . Clinical guide for the management of trauma and orthopaedic patients during the coronavirus pandemic. version 2 . 2020 . https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites /52/2020/03/C0274-Specialty-guide-Orthopaedic-trauma-v2-14-April.pdf (date last accessed 9 May 2020 ). Google Scholar
16. Xu S , Li Y . Beware of the second wave of COVID-19 . Lancet . 2020 ; 395 ( 10233 ): 1321 – 1322 . Crossref PubMed Google Scholar
17. NHS Highland . NHS near me . 2020 . https://www.nhshighland.scot.nhs.uk/ NHSNearMe/Pages/Welcome.aspx (date last accessed 15 June 2020 ). Google Scholar
18. British Orthopaedic Association . Information for BOA members on trauma and orthopaedic care in the UK during coronavirus pandemic . 2020 . https://www.boa.ac.uk/resources/information-for-boa-members-on-trauma-and-orthopaedic-care-in-the-uk-during-coronavirus-pandemic.html (date last accessed 12 June 2020 ). Google Scholar
Author contributions
A. S. Elhalawany: Designed the study, Collected and analyzed the data, Wrote the manuscript.
J. Beastall: Designed the study, Reviewed data collection and analysis, Reviewed and edited the manuscript.
G. Cousins: Designed the study, Reviewed and edited the manuscript.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
© 2020 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attributions licence (CC-BY-NC-ND), which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
