




Abstract
The number of clinical negligence claims in the UK is constantly increasing. As a specialty, trauma and orthopaedic surgery has one of the highest numbers of negligence claims.1 This study analyses NHS Litigation Authority (NHSLA) claims in trauma and orthopaedics between 2004 and 2014.
A formal request was made to the NHSLA under the Freedom of Information Act in order to obtain all data related to claims against orthopaedic surgery. It was found that the number of claims, and percentage of successful claims, has been constantly increasing over this period, with compensation paid of over £349 million.* Errors in clinical management accounted for the highest number of closed claims (2933 claims), costing over £119 million.*
The level of compensation paid out has a significant financial impact on the NHS. Reforms need to be made in order to tackle the high cost of legal fees generated by these claims, which further drain the limited resources available to the NHS.
INTRODUCTION
Medical malpractice frequently attracts a lot of attention in the press because it provokes headlines which sell newspapers. For a claim in clinical negligence to be valid, three criteria have to be fulfilled:
The claimant was owed a duty of care by the defendant
A breach of this duty occurred
Harm occurred to the plaintiff as a result of the breach in that duty of care.
The volume of claims resulting from clinical negligence cases has increased by 1200% over the last three decades,2 and costs the NHS vast amounts of money each year.3 The specialty of trauma and orthopaedics has the second highest rate of litigation in surgery.2 The number of surgical procedures performed in trauma and orthopaedics in the UK has also increased significantly in the last two decades.4
This paper analyses the data available from the National Health Service Litigation Authority (NHSLA), aiming to evaluate the trend in claims in this specialty, in order to highlight the areas in which orthopaedic consultants and trainees, together with nursing, physiotherapy and management staff, must focus in order to improve the quality of orthopaedic care and reduce the financial burden that negligence claims are causing to the NHS in the UK.
The number of complaints made to the General Medical Council has increased 15-fold since 1990.5 However, this approach of blame and retribution means that practitioners are not only less willing to accept their mistakes, but also less willing to highlight a fault of their colleague because of the fear that it might ruin his or her career. Legislation, by way of the Duty of Candour has been introduced to address this.
The NHSLA
The NHSLA was set up in 1995 as a Special Health Authority and a non–profit-making organisation of the Department of Health. Initially, its sole purpose was to ‘risk pool’ in terms of clinical claims arising as a result of incidents on or after1 April 1995.
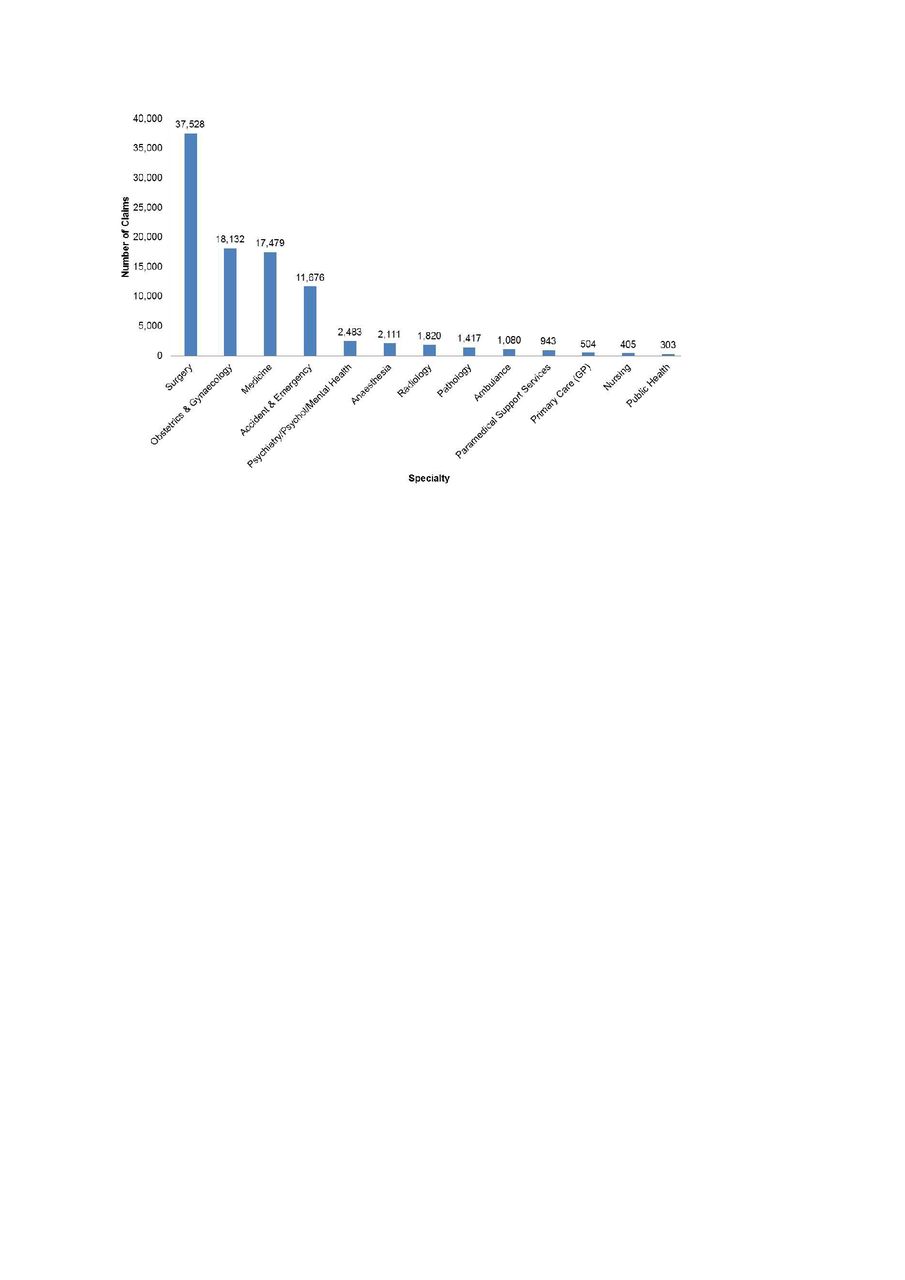
Fig. 1
FigCapTotal number of reported CNST claims by specialty (since the scheme began in April 1995).6
As we can see from the graph (Fig. 1), the NHSLA has managed over 95 000 claims since its inception. Over 37 000 of these have been in surgery (excluding obstetrics and gynaecology). During the 2013-2014 period, the NHSLA paid out over £262 million in clinical negligence claims. The NHSLA estimates that it has potential liabilities of £25.7 billion in relation to clinical negligence claims.7 This figure represents the estimated value of all known claims.
METHODS
The NHSLA has the remit to centralise and standardise all claims in the National Health Service. As an organisation, it has been notified of all claims since 2002. The study was a retrospective analysis of the NHSLA database to review all claims in trauma and orthopaedics, both in the emergency and elective setting.
A request was made under the Freedom of Information Act (2000), to obtain data of claims in trauma and orthopaedics in the ten years between 2004 and 2014. Data were obtained with yearly information on the category of the claim, number of claims, whether the claims were successful or not and, if successful, the amount paid out. These data were then analysed and collated in order to record the following information:
The category in which the claim fell, including the nature of the claim
Whether the claim is open or closed, and
The total cost paid for the claim if successful.
A request was also made following this, to obtain more clinical information regarding each claim, but unfortunately this was not made available by the NHSLA.
The data are presented below with the total costs quoted to the nearest £100. Claims that were not closed were not included in the final analysis.
RESULTS
It was found that during the period between 2004 and 2014, there were a total of 11 397 claims made to the NHSLA in trauma and orthopaedics; 8614 of these claims have been resolved, leaving 2783 claims which were unresolved. Hence, we can see that 75% of claims since 2004 have been resolved. Over 95% of the claims made each year prior to the 2010 to 2011 period had been resolved. The percentage of successful claims was just over 50% between 2004 and 2007. This increased to over 60% from 2007 onwards.*
Among the total number of resolved claims, 41% of them were unsuccessful while 59% of them were successful in claiming compensation with a total payout of £349,494,200. It should also be noted that2783 (24%) of the claims were still to be resolved. In the data provided by the NHSLA, legal costs were not accounted for as far as claimant costs were concerned. However, expenditure on clinical claims between 2013 and 2014 showed that, of the overall £1.193 billion spent on clinical negligence claims, 22% (£259 million) was spent on claimant solicitors compared with only 8% (£92 million) on defence legal costs.1 This shows a surprising discrepancy in claimant versus defence legal cost expenditure.
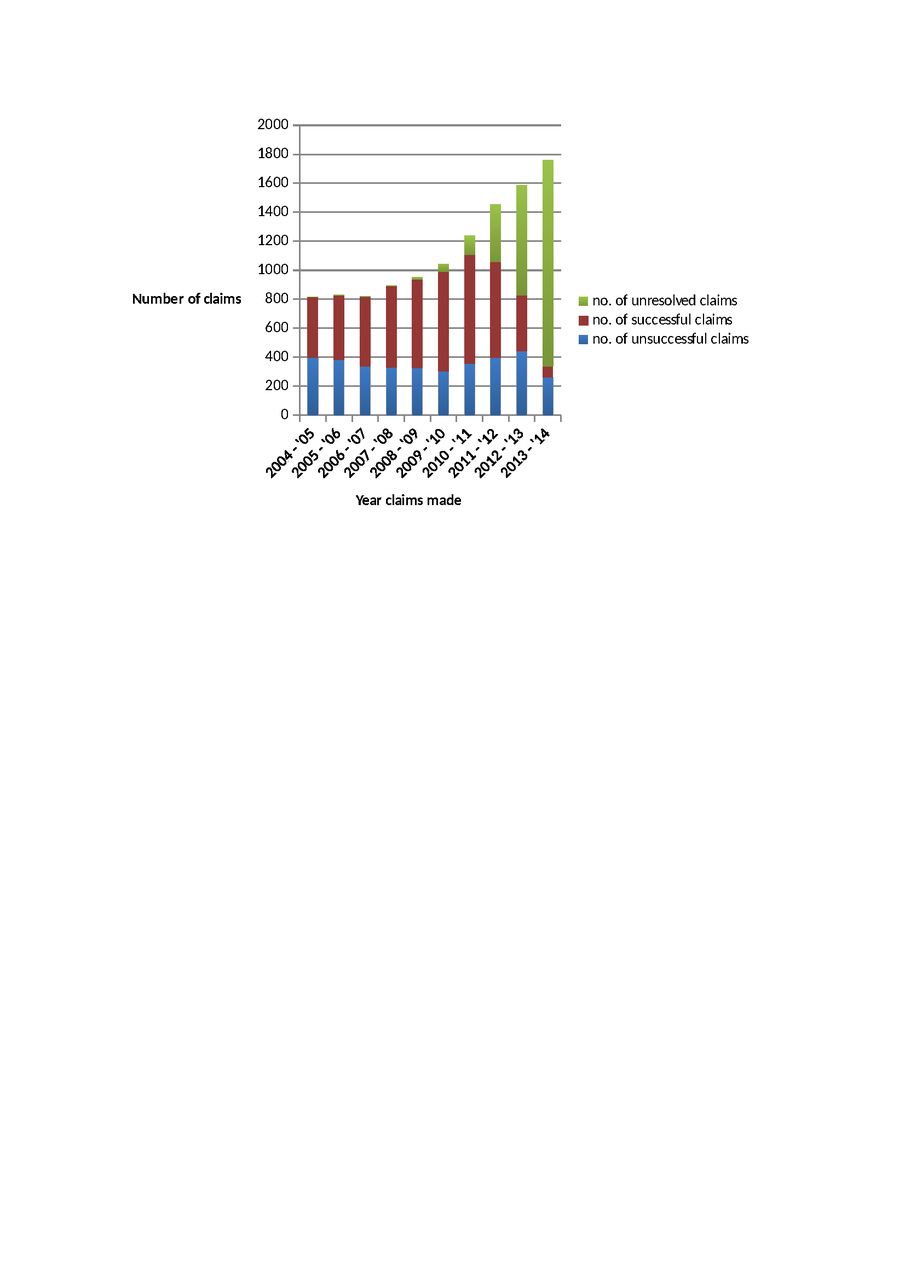
Fig. 2
Bar chart showing the trend in claims made to the NHSLA between 2004 and 2014.
The trend in the number of claims is seen in Fig. 2. The percentage of successful claims up until the 2009 to 2010 period was on the rise. It falls beyond this time, mainly because of the number of claims that currently remain unresolved. One can see that the overall number of claims is certainly on the rise. A total of 1758 claims were made to the NHSLA in the period 2013 to 2014; more than double the number from ten years earlier.
The percentage of successful claims (Fig. 3) shows a steady increase between 2004 and 2010. Beyond this, there is a decline in the percentage of successful claims when compared with unsuccessful claims. This is largely due to the fact that there are a large number of outstanding unresolved claims.

Fig. 3
Trend in the percentage of successful claims over the year.
Considering that 95% of claims prior to 2010 have been closed, it can be seen that from 2004 until 2009, the total amount paid out is steadily increasing. In 2004/2015 the total compensation for successful claims was £32 million. This increased up to 2008/9, with compensation of approximately £56 million. The overall compensation since then has declined but this is due to the fact that there are a large number of unresolved claims. In the 2012/2013 and 2013/2014 periods, there were over 1500 claims in each year, with 760 and 1421 unresolved claims in those years respectively.
Table I shows a breakdown of the number of claims over the ten-year period, and also the total amount of compensation paid out by NHSLA over this timeframe. During this period the mean payout for a successful case was £68,800. Table II shows the nature of the claims made, in terms of the area of clinical practice. It is interesting to note the number of claims relating to consent issues (320), which represents 4.5% of the total. Given the Supreme Court ruling in the Montgomery case earlier this year with the removal of the application of the Bolam principle from consent and the focus on a patient-orientated consent process, it will be interesting to see if consent claims increase in the next few years. It would be useful to have a better breakdown from the NHSLA of the categories “mismanagement” and “clinical care”, as in reality they are too vague to help us or our trainees and colleagues in avoiding claims against us.
Table I. Cost of litigation over the years
| Year | Unsuccessful claims | Successful claims | Unresolved claims | Percentage Successful | No. of claims | Paid out (£) |
|---|---|---|---|---|---|---|
| 2004-5 | 396 | 421 | 1 | 52 | 818 | £32,078,700 |
| 2005-6 | 383 | 446 | 1 | 54 | 830 | £33,899,100 |
| 2006-7 | 336 | 479 | 5 | 59 | 820 | £44,123,600 |
| 2007-8 | 330 | 561 | 4 | 63 | 895 | £49,255,700 |
| 2008-9 | 327 | 610 | 16 | 65 | 953 | £55,924,600 |
| 2009-10 | 303 | 688 | 51 | 69 | 1042 | £48,284,700 |
| 2010-11 | 356 | 753 | 130 | 68 | 1239 | £48,542,800 |
| 2011-12 | 398 | 662 | 394 | 62 | 1454 | £26,653,200 |
| 2012-13 | 444 | 384 | 760 | 46 | 1588 | £9,884,400 |
| 2013–14 | 261 | 76 | 1421 | 23 | 1758 | £847,400 |
| Total | 3534 | 5080 | 2783 | 59 | 11397 | £349,494,200 |
Table II. Cost of litigation by claim category
| Claim category | No. of closed claims | No. of unsuccessful claims | No. of successful claims | Percentage successful claims | Mean Cost | Total Cost |
|---|---|---|---|---|---|---|
| Mismanagement | 2933 | 1358 | 1575 | 53 | £75,600 | £119,061,700 |
| Intra-operative injury | 1437 | 606 | 831 | 57 | £83,600 | £69,501,708 |
| Diagnosis | 1337 | 542 | 795 | 59 | £81,600 | £64,860,900 |
| Patient care | 848 | 316 | 532 | 62 | £37,900 | £20,186,978 |
| Consent | 320 | 142 | 178 | 55 | £77,200 | £13,745,400 |
| Infection | 140 | 83 | 57 | 40 | £79,100 | £4,506,000 |
| Wrong site surgery | 66 | 4 | 62 | 93 | £18,600 | £1,152,000 |
Mismanagement
The highest category in which claims were paid out was that of ‘mismanagement’, with total compensation of over £119 million. There were 2933 closed claims in this category with 1575 of them being successful. Claims in this category included a delay due to inappropriate investigations being performed, and hence resulting in a delay in administering the appropriate treatment. This was a relatively broad category which covered a lot of claims with precious little clinical information for most of these cases.
Intra-operative injury
The next category was intra-operative injury with over £69 million paid out in compensation. This included all cases where the successful claim was a result of an intra-operative injury or complication during the procedure. It also resulted in the highest mean cost per successful case (£83,600) and 57% of the claims in this category were successful over the period studied.
Diagnosis
This category has the second highest overall level of compensation for successful claims. It included cases where the diagnosis had been missed, delayed or an incorrect diagnosis was made. It resulted in compensation slightly less than was paid out for intra-operative injuries, of approximately £65 million. The percentage of successful claims within this category was also (comparatively) higher than most others at 59%.
Patient care, consent and infection
The numbers in Table II relate to litigation concerning patient care, consent and infection. Both the categories of consent and infection had comparatively high mean payout costs. However, it is noted that claims made on the basis of infection were only successful on 40% of occasions.
Wrong site surgery
The World Health Organisation (WHO) Surgical Checklist was published in 2008 and implemented in Trusts across the UK by the following year. Appropriate use of the checklist in the operating theatre should have reduced the number of ‘never events’ such as wrong site surgery. There were 66 settled claims in this category over the last ten years, with an understandably high success rate of 93%. This resulted in compensation of over £1.1 million in the period reviewed. Fifty-six of the 66 claims occurred up until the year 2009/10. The number of claims has reduced following the introduction of the WHO checklist, with only ten such claims being made in the last four years.
DISCUSSION
The overall level of compensation paid out for orthopaedic and trauma surgery in the last ten years has been more than £349 million. The three-year statute of limitation and the average duration of a claim prevent us from comprehensively examining the data in the last five years of the study.
Litigation specific to trauma and orthopaedics is growing when compared with other specialties across the NHS, and this is clearly an issue that needs to be addressed. One of the main reasons behind this is the fact that limb surgery is potentially high risk, and complications are therefore inevitable. It can also be explained by the fact that there has been a dramatic increase in the number of procedures performed in trauma and orthopaedics over the last ten years. There were approximately 185 433 joint arthroplasties performed in England, and a further 10 860 performed in Wales alone in 2012/13. This has risen by 7.5% when compared with the previous year. Over 1.2 million hip and knee arthroplasties were performed in the UK between the years of 2003 and 2013.
A significant limitation of the study was that a more detailed clinical picture of individual claims was not made available because of restrictions under the Freedom of Information Act. It should be noted that the NHSLA data were collected purely for legal/administrative/cost purposes and not for research analysis. Therefore, despite being provided with the data for every year, including the number of claims under the various categories, there is insufficient clinical detail available to draw definite conclusions about specific areas of clinical practice. It would certainly be more instructive if such information was available. This makes it difficult to specifically analyse the available data and runs a risk of either under-reporting, or reporting within the wrong category. The statistics reported in this study are collected to detect trends in litigation rather than detect specific procedures that are high risk. A lot of the claims were also entered under two or three different categories due to the complex nature of the claim. These were then re-categorised based on the nature of the primary claim.
The total number of claims due to “mismanagement” was 2933, with the mean cost of claims being £75,600. This was less than the amount paid out for intra-operative injury (£83,600) and claims related to delay, and missed or wrong diagnosis (£81,600). Studies have reported that in relation to ‘misdiagnosis’, the most common causes were fractures and dislocations that were missed in the emergency department.8,9
CONCLUSION
There are a number of reasons why there is an overall increase in the trend towards litigation in England and Wales. Society as a whole is becoming increasingly medically aware. Solicitors and claims agencies now openly advertise in the press and on TV, inviting people who have any problems after medical intervention to have a free, no obligation appointment to see if a negligence claim is likely to be successful, and will often run claims on a ‘no-win-no-fee’ basis, or with after-the-event insurance if an expert screening report indicates that there may be a case. Indeed, on occasions some patients are encouraged to pursue claims that have little chance of success in the hope and expectation that the Trust or NHSLA will make an ‘economic’ settlement of a few thousand pounds to get it off their books and avoid expenses on expert reports and further legal fees. The increasing media coverage of a minority of complications or errors and the sensationalism of the same has diminished the faith that the general public have in the healthcare system. These, along with the payment of large sums of money for successful claims, have led to an increasingly litigious culture. Many patients therefore want (and are encouraged) to pursue legal action at every available opportunity.
The role of the NHSLA in risk pooling and now managing all claims has certainly made the claims process more efficient. Data are being managed in order to develop strategies to limit litigation. Hence, we can see that more cases are being managed by mediation and an increasing number are being settled out of court.
As discussed, issues of consent are also a cause of complaint in a lot of cases. However, taking the time to consent in the outpatient setting rather than rushing it on the day of the procedure significantly reduces the risk of litigation, as reported by Bhattacharya et al in their study on ‘informed consent’.10 However, the impact of the Montgomery ruling may take two or three years to become apparent through the NHSLA records.
Having looked at the data above, one must conclude that a large sum of money is being spent on malpractice in the NHS in the UK. This is disappointing considering the tight budget and the increasing demands of a growing ageing population. Having said that, there are tragic cases and mistakes made for which individuals should be compensated. However, not all systems are perfect and it may appear that we are overspending in clinical negligence cases. It is difficult to be sure if this is due to increasing errors and substandard care or overzealous solicitors who want to make the most that they can of an incident for their clients. Looking at alternative systems, it seems that it would be impossible to find a system that holds professionals who have been negligent responsible for their actions whilst at the same time encouraging openness and an environment where everyone learns from previous mistakes. Perhaps it is time to revisit the question of a ‘no fault’ compensation scheme for medical accidents, as exists in New Zealand, Sweden, Finland and Denmark. The Scottish government have been investigating such a scheme (based on the Swedish model) for the last five years and now intend to proceed with caution, and further explore how the system may work.
ENDNOTE
*Data obtained by the author from the NHS Litigation Authority, under the Freedom of Information Act.
1 No authors cited. NHS Litigation Authority report and accounts 2013/14. http://www.nhsla.com/aboutus/Documents/NHS%20LA%20Annual%20Report%20and%20Accounts%202013-14.pdf (date last accessed 2 November 2015). Google Scholar
2 No authors listed. The NHS Litigation Authority factsheet 3: information on claims 2014-2015. http://www.nhsla.com/currentactivity/Documents/NHS%20LA%20Factsheet%203%20-%20claims%20information%202014-15.pdf (date last accessed 4 November 2015). Google Scholar
3 Harpwood V. Medicine, malpractice and misapprehensions. Abingdon: Routledge-Cavendish, 2007). Google Scholar
4 No authors listed. National Joint Registry NJR stats online. http://www.njrcentre.org.uk/njrcentre/Healthcareproviders/Accessingthedata/StatsOnline/tabid/117/Default.aspx (date last accessed 4 November 2015). Google Scholar
5 No authors listed. General Medical Council: the state of medical education and practice in the UK. http://www.gmc-uk.org/SOMEP_2013_web.pdf_53703867.pdf (date last accessed 4 November 2015). Google Scholar
6 No authors listed. The NHS Litigation Authority factsheet 2: financial information. http://www.nhsla.com/currentactivity/Documents/NHS%20LA%20Factsheet%202%20-%20financial%20information%20-%202014-15.pdf (date last accessed 15 October 2015). Google Scholar
7 No authors listed. Department of Health annual report and accounts 2014-15. https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/447002/DH_accounts_14-15_web.pdf (date last accessed 16 November 2015). Google Scholar
8 Atrey A, Gupte CM, Corbett SA. Review of successful litigation against English health trusts in the treatment of adults with orthopaedic pathology. J Bone Joint Surg [Am] 2010;92-A:e36. Google Scholar
9 Machin JT, Briggs TWR. Litigation in trauma and orthopaedic surgery. Journal of Orthopaedics and Trauma 2014;2:32. Google Scholar
10 Bhattacharya T, Yeon H, Harris MB. The medical-legal aspects of informed consent in orthopaedic surgery. J Bone Joint Surg [Am] 2005;87-A:2395-2400. Google Scholar
