




Newly described1 (and ‘rounded up’) in this edition of 360, sternoclavicular joint arthroscopy is likely to be an emerging surgical technique. The sternoclavicular joint (SCJ) has not previously been a particular focus of operative interest to the orthopaedic fraternity. Operative intervention for traumatic posterior dislocations with potential mediastinal or vascular compromise is usually indicated, but there is no consensus with regards to the operative management of acute anterior dislocations or atraumatic instability. Intra-articular pathology, mainly in the form of osteoarthritis or a disc tear, is usually treated with various types of anti-inflammatory medications, analgesia or physiotherapy and the potential for surgical intervention has been at best considered as a last resort, although the results, from the limited studies available, have actually been uniformly good.
An arthroscopic approach to the sternoclavicular joint has not previously been described but could potentially offer the ability to access the joint surgically without the risk of damage to the great vessels and surrounding structures. With the newly described arthroscopic approach the patient is positioned supine with a sandbag between their scapulae to push the sternum forward, effectively opening up the anterior SCJ. The rationale for the positioning of superior and inferior portals to avoid damage to the anterior sternoclavicular ligament and the angle of inclination required to enter the joint parallel to the sternal articular surface are described. An 18-gauge spinal needle is initially inserted into the inferior joint which is then filled with normal saline. A flashback indicating that the needle is in the joint. A 3.5 mm mini trocar is then inserted into the joint and a 2.9 mm arthroscope introduced. Once safely in the joint, the posterior capsule can always be kept in view allaying any concerns regarding damage to the posterior mediastinal structures. A superior working portal is then established under direct vision, again using the spinal needle. An initial diagnostic arthroscopy is recommended to assess the central disc (which is usually degenerate and torn) and the clavicular and sternal articular surfaces. If the disc is complete the arthroscope needs to be inserted on either side.
Using mini-instruments, a mini-shaver and mini-radiofrequency probe, 50 operative therapeutic cases are described in the article. The majority of these have been for SCJ osteoarthritis and have involved excision of the medial end of the clavicle (Figs 1 & 2). Having evolved the technique the most successful results can be obtained through excision of the articular cartilage and chondral bone back to cancellous bone, but care should be taken to resect no more than 5 mm which gives better results than a more extensive resection. The article also details operative interventions for SCJ disc pathology. This includes three cases in younger patients with acute disc tears and ongoing clicking and pain, diagnosed by MRI, that have responded well to excision and a further six patients with more chronic symptoms and a degenerate tear, which can be differentiated at arthroscopy, who have also responded equally well.
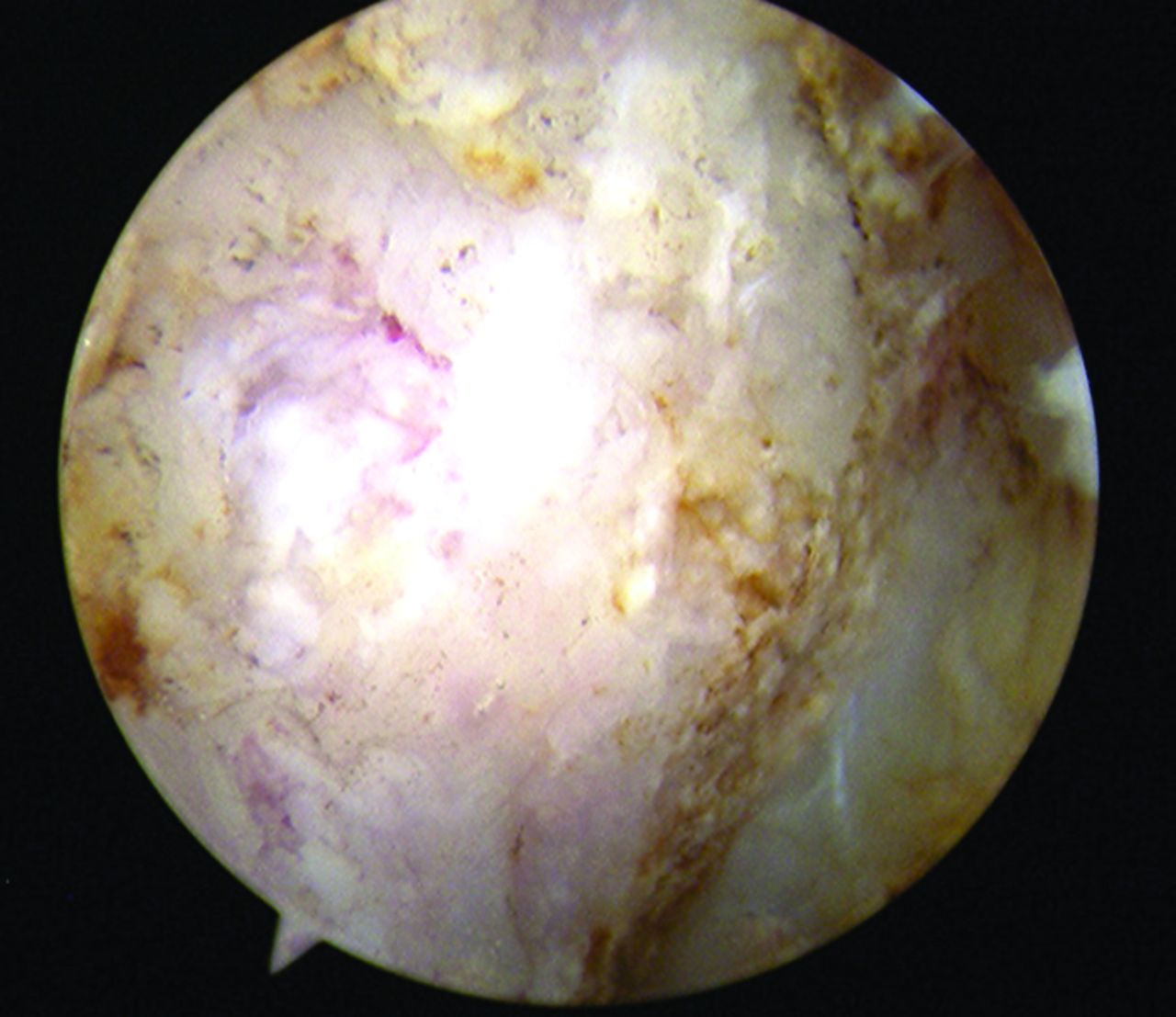
Fig. 1
Arthroscopic view of the medial end of right degenerated clavicle.
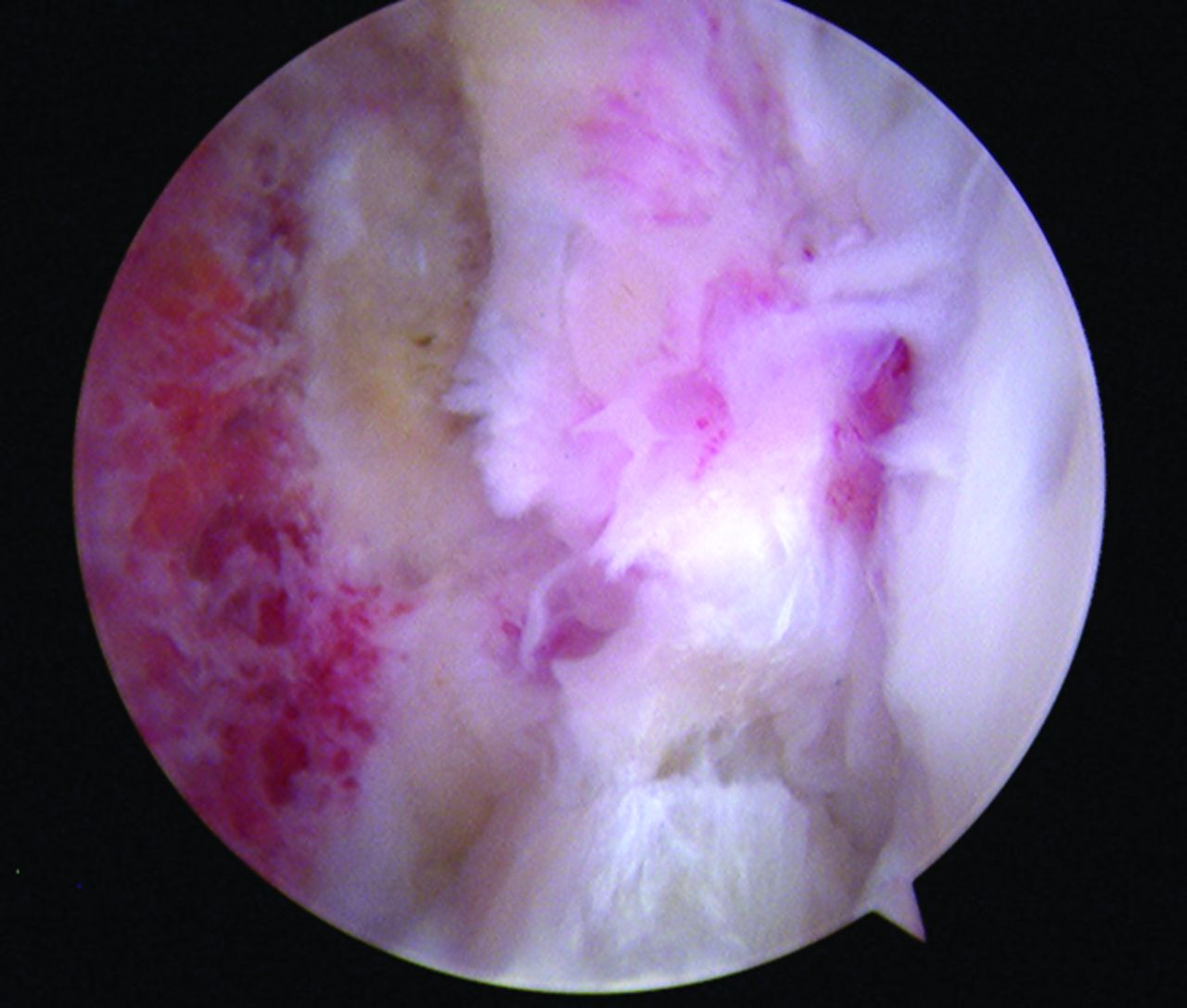
Fig. 2
View after excision of the medial end of the clavicle with the resected rim of the sternoclavicular disc and the relatively preserved sternal articular cartilage.
The surgery is usually performed as a day case and patients require no post-operative immobilisation. No complications have been reported, particularly with regard to instability, scarring or vascular injury.
On the face of it, SCJ arthroscopy does appear to be a viable procedure but it will be interesting to see whether this is something that will be taken up by other surgeons. SCJ arthroscopy is not a particularly challenging technical procedure but due mainly to the relative rarity of pathology, is only likely to be taken up in larger referral centres. In the current climate it is rare for a completely new and innovative procedure to be described and a certain pioneering spirit is, after all, required.
1 Tytherleigh-Strong G . Arthroscopy of the sternoclavicular joint. Arthrosc Tech2013;2:E141–E145.CrossrefPubMed Google Scholar
