




Abstract
Objectives
This study evaluated the mechanical performance, under low-load cyclic loading, of two different knotless suture anchor designs: sutures completely internal to the anchor body (SpeedScrew) and sutures external to the anchor body and adjacent to bone (MultiFIX P).
Methods
Using standard suture loops pulled in-line with the rotator cuff (approximately 60°), anchors were tested in cadaveric bone and foam blocks representing normal to osteopenic bone. Mechanical testing included preloading to 10 N and cyclic loading for 500 cycles from 10 N to 60 N at 60 mm/min. The parameters evaluated were initial displacement, cyclic displacement and number of cycles and load at 3 mm displacement relative to preload. Video recording throughout testing documented the predominant source of suture displacement and the distance of ‘suture cutting through bone’.
Results
In cadaveric bone and foam blocks, MultiFIX P anchors had significantly greater initial displacement, and lower number of cycles and lower load at 3 mm displacement than SpeedScrew anchors. Video analysis revealed ‘suture cutting through bone’ as the predominant source of suture displacement in cadaveric bone (qualitative) and greater ‘suture cutting through bone’ comparing MultiFIX P with SpeedScrew anchors in foam blocks (quantitative). The greater suture displacement in MultiFIX P anchors was predominantly from suture cutting through bone, which was enhanced in an osteopenic bone model.
Conclusions
Anchors with sutures external to the anchor body are at risk for suture cutting through bone since the suture eyelet is at the distal tip of the implant and the suture directly abrades against the bone edge during cyclic loading. Suture cutting through bone may be a significant source of fixation failure, particularly in osteopenic bone.
Cite this article: Y. Ono, J. M. Woodmass, A. A. Nelson, R. S. Boorman, G. M. Thornton, I. K. Y. Lo. Knotless anchors with sutures external to the anchor body may be at risk for suture cutting through osteopenic bone. Bone Joint Res 2016;5:269–275. DOI: 10.1302/2046-3758.56.2000535.
Article focus
-
This study evaluated the mechanical performance, under low-load cyclic loading, of different knotless suture anchor designs: sutures completely internal to the anchor body (e.g. SpeedScrew, ArthroCare Corp., Austin, Texas) and sutures external to the anchor body and adjacent to bone (e.g. MultiFIX P, ArthroCare).
-
Mechanical performance of knotless suture anchors that have sutures external to the anchor body was hypothesised to be inferior to that of anchors with sutures completely internal to the anchor body.
-
Mechanical performance of knotless suture anchors that have sutures external to the anchor body was hypothesised to be affected by bone quality.
Key messages
-
Anchors that had sutures external to the anchor body exhibited inferior mechanical performance compared with anchors that had sutures completely internal to the anchor body.
-
Suture cutting through bone was more pronounced throughout cyclic loading in anchors that had sutures external to the anchor body compared with anchors that had sutures completely internal to the anchor body.
-
Anchors with sutures external to the anchor body and directly against bone are at risk for suture cutting through bone particularly in patients with osteopenic bone.
Strengths and limitations
-
Mechanical performance of knotless suture anchors was evaluated in cadaveric bone and three foam blocks representing bone quality from normal to osteopenic.
-
‘Suture cutting through bone’ was evaluated using video recordings of mechanical tests.
-
Bone quality of cadaveric bone was not measured quantitatively.
Introduction
Rotator cuff tears are the most common cause of pain in the adult shoulder. The prevalence of rotator cuff tears increases with age and over half of the population older than 60 years are reported to have some degree of rotator cuff tearing even in shoulders without symptoms.1 Surgical repair of torn rotator cuff tendons is currently an option for individuals who have failed conservative treatment. While the clinical results are relatively successful, re-tear rates following rotator cuff repair have been reported to be as high as 10% to 90%.2 In addition, patients older than 60 years have lower healing rates than younger patients due to a multitude of factors.3 Poor biological healing potential may be an important factor in older patients. However, failure of mechanical fixation may also be a critical factor and can be directly influenced by the surgeon. In this elderly population, surgeons are faced with not only poor soft-tissue quality but also poor bone quality when performing rotator cuff repair.
Over the last few decades, surgical procedures for rotator cuff tendon fixation to bone have evolved dramatically.4 Originally, open transosseous techniques were the benchmark in rotator cuff repair where sutures were passed through bone tunnels and the tendon was tied directly onto the greater tuberosity. Eventually suture anchors were developed which allowed firm fixation of sutures to the bone. These ‘traditional’ suture anchors had multiple pairs of sutures attached to the anchor, which allowed the procedure to be performed arthroscopically, but still required the complex surgical task of arthroscopic knot tying. With the advent of knotless suture anchors,5 various designs were developed with different methods of anchor fixation and suture locking mechanisms.5-10
Knotless suture anchors can generally be divided into two major designs according to the way the sutures are handled with respect to the anchor body. Internal knotless suture anchors have sutures which are completely internal to the anchor body while external knotless suture anchors have sutures (on the side of loading) external to the anchor body (Fig. 1).11 Furthermore, internal knotless suture anchors, e.g. SpeedScrew anchor (ArthroCare Corp., Austin, Texas), typically have a suture locking system completely internal to the anchor body, whereas the external knotless suture anchors, e.g. MultiFIX P anchor (ArthroCare), at least partially rely on an interference suture locking mechanism between anchor surface and bone. Since the suture locking mechanism relies on an interference fit between the anchor and bone, our previous studies have demonstrated that external knotless suture anchors may be at risk for loss of tendon fixation particularly in osteopenic bone.11

Fig. 1
Two major designs of knotless suture anchors according to the way the sutures are handled with respect to the anchor body: (left) internal knotless suture anchor (e.g. SpeedScrew anchor), (right) external knotless suture anchor (e.g. MultiFIX P anchor).
In addition, many of these external knotless suture anchor design have a suture eyelet, which is distal on the anchor body (Fig. 1). This eyelet position may predispose the anchor-suture construct to failure, as under cyclic loading, the sutures may abrade against the adjacent bone resulting in the suture cutting through bone.
As far as we are aware, no study has demonstrated this possible effect of suture cutting through bone and compared the difference between the two major anchor designs (internal and external), either in experimental or clinical settings. Understanding possible unfavorable effects specific to anchor designs will help surgeons use appropriate anchors in rotator cuff repair considering variable aspects (e.g., bone quality, type of repair construct, area of anchor placement).
Therefore, the purpose of this study was to evaluate the mechanical performance of these two types of knotless anchors: sutures completely internal to the anchor body and sutures external to the anchor body and adjacent to bone, in particular focusing on the suture cutting through bone. Foam blocks with different densities were used in addition to cadaveric bones to isolate the effect of bone quality. We hypothesised that the external knotless suture anchors would demonstrate more suture cutting through bone than internal knotless suture anchors and that this would be affected by bone quality.
Materials and Methods
Knotless suture anchors
Anchors tested were 5.5 mm SpeedScrew and 4.5 mm MultiFIX P representing an internal and external anchor, respectively. Both anchors were tested in human cadaveric humeral heads and foam blocks.
Cadaveric bone
In order to simulate the clinical condition of the shoulder following a rotator cuff repair, eight anchors of each design were randomly inserted into the tuberosities of six paired cadaveric specimens (46 years to 55 years), with a deadman’s angle (i.e. 45°)12 until the horizontal laser line was flush to the bone surface. All anchors were tested using a standard suture loop (40.5 mm length) and pulled in-line with the rotator cuff (approximately 60°).
Mechanical tests were performed using a Lloyd LRX Plus with a 1000 N load cell and NEXYGEN Plus 3.0 software (both Lloyd Materials Testing, West Sussex, United Kingdom). Mechanical testing was preloading and cyclic loading. Preloading to 10 N at 60 mm/min was followed by holding the preload of 10 N for ten seconds. Cyclic loading was 500 cycles from 10 N to 60 N at 60 mm/min.13
The parameters evaluated were the initial displacement from the preload (10 N) to the peak (60 N) of the first cycle and the cyclic displacement from the peak of the first cycle to the peak of the 500th cycle. In addition, the number of cycles and the load at 3 mm displacement relative to the preload were determined. If the displacement relative to the preload did not exceed 3 mm after 500 cycles, then the number of cycles at 3 mm displacement relative to the preload was 500 and the load at 3 mm displacement relative to the preload was 60 N. Video recording was used throughout the tests for all the tested anchors to document the predominant source of suture displacement.
Foam blocks
To evaluate the effect of suture cutting through the bone, the two anchors (5.5 mm SpeedScrew, 4.5 mm MultiFIX P) were further tested in foam blocks representing a spectrum of bone quality from normal to osteopenic bone (i.e. 20/8, 15/8, 8/8 foam). Individual anchors were tested in individual polyurethane foam bone blocks (General Plastics Manufacturing Co., Tacoma, Washington) where 20/8 foam had a 3 mm 20 pcf (pounds per cubic foot) layer laminated on a 8 pcf block, 15/8 foam had a 3 mm 15 pcf layer laminated on a 8 pcf block and 8/8 foam was a 8 pcf block. In all, five samples of each foam and anchor combination were tested. To simulate the pull of the rotator cuff, all anchors were inserted at an angle of 90° to the foam surface and then tested through suture loops (40.5 mm length) pulling at 60° from the axis of the anchor. The mechanical testing protocol and parameter definitions were similar for the foam blocks tests and cadaveric bone test as described previously. Video from a standardised top-down view was recorded for all anchors tested in 15/8 foam and distances of ‘suture cutting through bone’ were visually measured using a ruler with 1 mm increments placed beside each individual anchor. Video recording was also used to document the predominant source of suture displacement.
Statistical analysis
In all, four samples were sufficient to detect a difference in the means of 1 mm with a standard deviation (sd) of 0.5 mm (alpha = 0.05 and power = 0.80; STATA 11.0, StataCorp, College Station, Texas). Based on this a priori power analysis, groups were allocated a minimum of five samples. Data were analysed using Kruskal-Wallis tests with Conover post hoc analysis when not normally distributed or analysis of variance (ANOVA) with linear contrasts when normally distributed.
Results
Cadaveric bone
In human bone, all of the SpeedScrew and MultiFIX P anchors completed the loading protocol. Initial displacement was greater for the MultiFIX P anchors than the SpeedScrew anchors (p < 0.05; Fig. 2a). Cyclic displacement was greater for the MultiFIX P anchors than the SpeedScrew anchors (p < 0.05; Fig. 2b). All of the MultiFIX P anchors reached 3 mm of displacement relative to the preload before reaching the peak of the first cycle (Fig. 2c). The number of cycles and load at 3 mm displacement relative to the preload were greater for the SpeedScrew anchors than the MultiFIX P anchors (p < 0.05; Figs 2c and 2d). Qualitative video analysis revealed a large amount of ‘suture cutting through bone’ even with the initial cycle, particularly by MultiFIX P anchors, whereas SpeedScrew anchors did not show as much displacement. Thus, ‘suture cutting through bone’ was considered to be the predominant source of suture displacement.
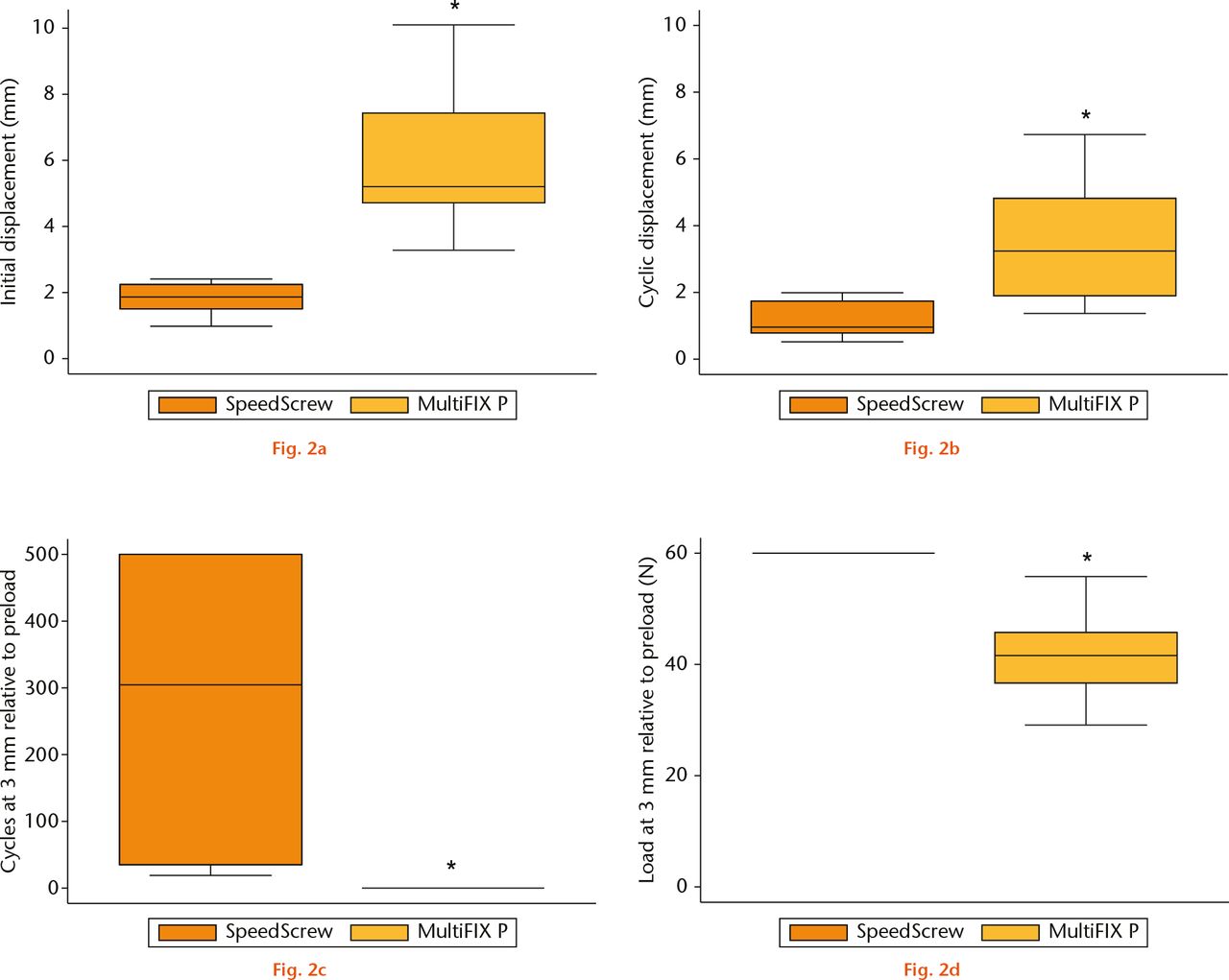
Fig.
Mechanical performance of knotless suture anchors in cadaveric bone: a) initial displacement from the preload to the peak of the first cycle; b) cyclic displacement from the peak of the first cycle to the peak of the 500th cycle; c) number of cycles at 3 mm displacement relative to the preload; d) load at 3 mm displacement relative to the preload.*MultiFIX P different than SpeedScrew (p < 0.05; analysis of variance or Kruskal-Wallis tests).
Foam blocks
Data from two tests were not analysed due to technical errors: one SpeedScrew in 8/8 foam and one MultiFIX P in 20/8 foam.
In osteopenic foam (8/8 foam), four out of five MultiFIX P anchors failed during cyclic loading by anchor pullout; whereas no SpeedScrew anchors failed out of four tested (p < 0.05; Fisher’s exact test). The initial displacement was greater for MultiFIX P anchors compared with SpeedScrew anchors (p < 0.05; Fig. 3a) but data for cyclic displacement was available for only one MultiFIX P anchor due to the anchor failure of the remaining MultiFIX P anchors (Fig. 3b). The number of cycles and load at 3 mm displacement relative to the preload were greater for the SpeedScrew compared with the MultiFIX P anchors (p < 0.05; Figs 3c and 3d).
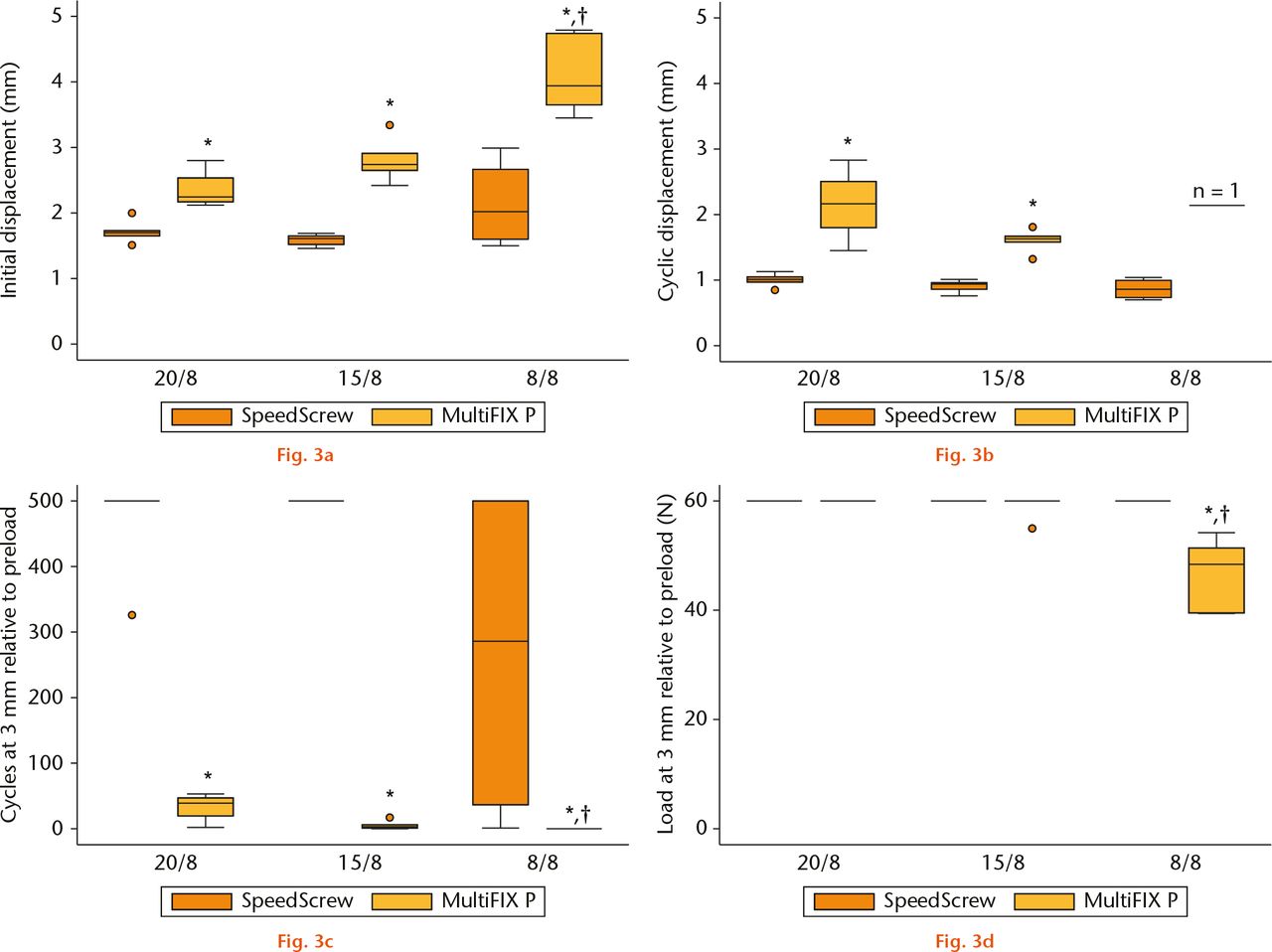
Fig.
Mechanical performance of knotless suture anchors in foam (20/8, 15/8, 8/8): a) initial displacement from the preload to the peak of the first cycle; b) cyclic displacement from the peak of the first cycle to the peak of the 500th cycle; c) number of cycles at 3 mm displacement relative to the preload; d) load at 3 mm displacement relative to the preload. “n = 1” indicates one observation because four out of five MultiFIX P anchors in 8/8 foam failed during cyclic loading.*MultiFIX P different than SpeedScrew (p < 0.05; analysis of variance (ANOVA) or Kruskal-Wallis tests).† 8/8 foam different than 15/8 foam and 20/8 foam (p < 0.05; ANOVA with linear contrasts or Kruskal-Wallis tests with Conover post hoc analysis).
In 15/8 foam and 20/8 foam, both initial and cyclic displacement were greater for MultiFIX P compared with SpeedScrew anchors (p < 0.05; Figs 3a and 3b). In 15/8 foam and 20/8 foam, the number of cycles at 3 mm displacement relative to the preload was greater for the SpeedScrew compared with the MultiFIX P anchors (p < 0.05; Fig. 3c); however, there was no statistical difference in the load at 3 mm displacement relative to the preload (Fig. 3d).
Comparing the different foams, SpeedScrew anchors were not affected by bone quality for any of the four parameters evaluated (Fig. 3). MultiFIX P anchors had greater initial displacement in 8/8 foam compared with both 15/8 and 20/8 foam (p < 0.05; Fig. 3a). Likewise, the number of cycles and load at 3 mm displacement relative to the preload were less for MultiFIX P anchors in 8/8 foam compared with both 15/8 and 20/8 foam (p < 0.05; Figs 3c and 3d).
Video analysis of the 15/8 foam block tests revealed significant ‘suture cutting through bone’ as a predominant source of suture displacement, especially during initial cycles (Fig. 4). ‘Suture cutting through bone’ was greater for MultiFIX P than SpeedScrew anchors at all of the various cycles evaluated (p < 0.05; Fig. 4).
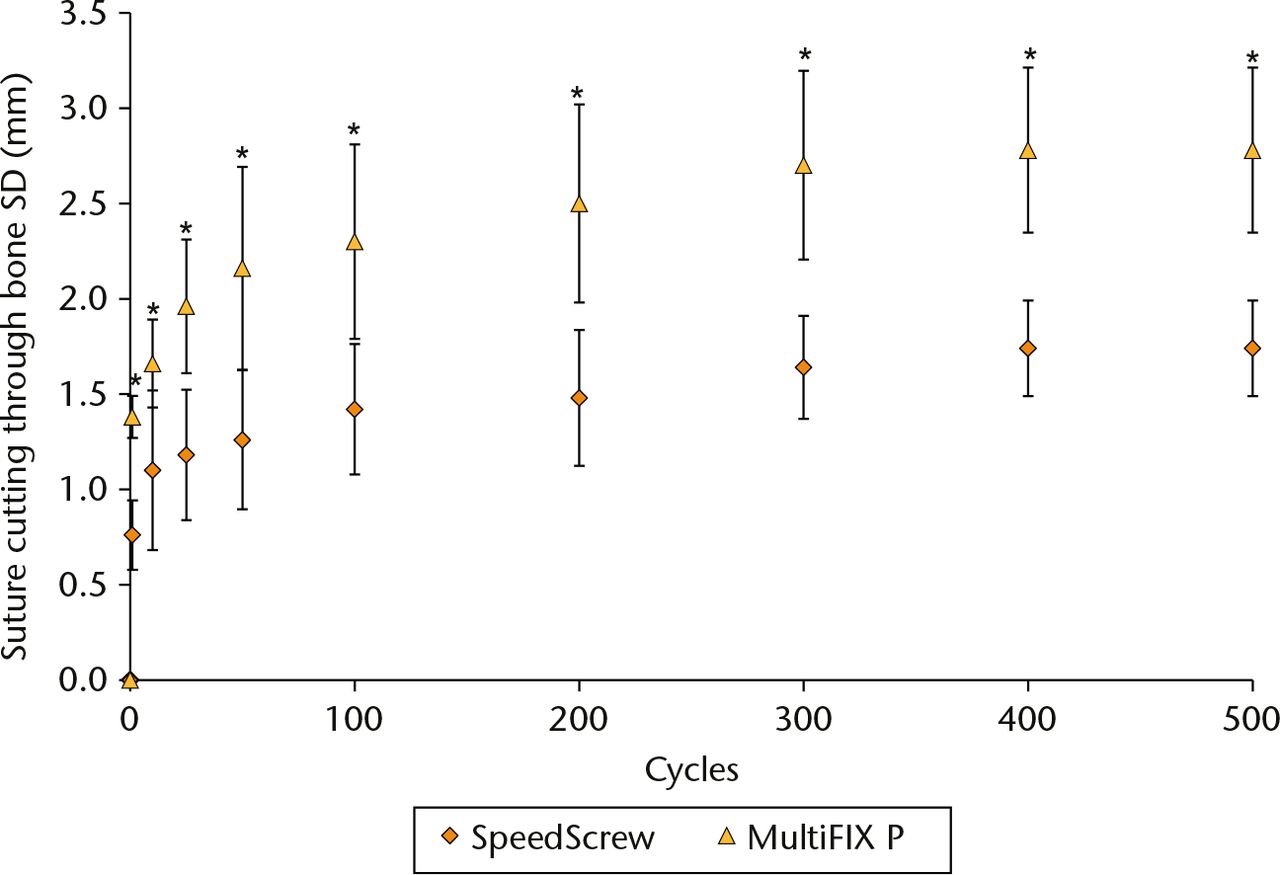
Fig. 4
‘Suture cutting through bone’ during cyclic loading of knotless suture anchors in 15/8 foam.*MultiFIX P different than SpeedScrew (p < 0.05; analysis of variance). sd, standard deviation.
Discussion
The current study confirmed our hypothesis that knotless suture anchors (where the sutures are external to the anchor body) have inferior mechanical performance when compared with anchors where the sutures are completely internal to the anchor body. This study demonstrated that the greater suture displacement in the ‘external’ type anchors was predominantly due to ‘suture cutting through bone’, which was enhanced in an osteopenic bone model.
There are a number of different factors which are important in suture anchor-based constructs for secure tendon fixation to bone (e.g. anchor fixation in bone, suture fixation to tendon, knot security, loop security).14 For example, poor bone quality has been linked with decreased pullout strength of suture anchors in cadaveric15-18 and foam models.16 Therefore clinically, care should be taken when placing anchors in osteopenic bone. Similarly, in the current study, the MultiFIX P anchors showed more frequent anchor pullout failures in earlier cycles in the osteopenic bone model than in the healthier bone models, which was consistent with Pietschmann et al.8 According to their study, maximum failure load decreased when comparing osteopenic humeri with healthy humeri for both SwiveLock and PushLock anchors, which are both external anchors. Although the purpose of the study from Pietschmann et al8 was to investigate the effect of bone mineral density on anchor-to-bone fixation, their findings led to the speculation that anchors with suture-to-anchor fixation dependent on interference between anchor and bone were affected by bone mineral density. The findings of the current study support this previous speculation regarding external anchors. Furthermore, our findings demonstrate that ‘suture cutting through bone’ was the predominant suture displacement for external anchors.
While the bone-anchor interface is critical for anchor fixation in bone, in external anchors, the bone-anchor interface is also critical for suture locking and therefore, any compromise to the bone-anchor interface may also affect knot security and loop security.14 Furthermore, in this study we also demonstrated that the MultiFIX P anchors had more suture displacement and suture cutting through bone at earlier cycles in an osteopenic bone model. This tendency was not observed with SpeedScrew anchors. Interestingly, this mode of failure has previously been described when transosseous rotator cuff repair constructs have been tested under cyclic loading. The transosseous method similarly relies on the lateral bone of the greater tuberosity for fixation. Under cyclic loading it has been shown that the suture can cut through the weak metaphyseal bone leading to tendon displacement and construct failure.19
We believe that the MultiFIX P anchor and, indeed, many external knotless anchors of similar design (e.g. PushLock, SwiveLock) are predisposed to a similar failure mechanism. These external anchors are not only reliant on the bone-anchor interface for suture locking, but also have a suture eyelet positioned distal on the anchor. Therefore, under loading conditions, these designs expose the entire suture length against the bone (along the medial aspect of the anchor hole) and can lead to suture cutting through bone. This is in contrast to the SpeedScrew anchor (i.e. internal knotless anchor) where the sutures are routed through the internal aspect of the anchor. These anchors minimise any suture exposure to the bone (along the medial aspect of the anchor hole) and, therefore, the effect of suture cutting through the bone. Furthermore, the anchor body itself may reinforce the medial aspect of the anchor hole and be protective to this potentially detrimental effect.
When a suture abrades against the adjacent bone (e.g., in external knotless suture anchors), this cannot only lead to loss of knot and loop security, but also breakage of the surrounding bone and enlargement of the anchor hole; this could result in loss of anchor stability and early catastrophic anchor failure (i.e. anchor pullout). Indeed, four of the MultiFIX P anchors pulled out early during cyclic loading in our osteopenic foam model. Each of these factors (i.e. knot security, loop security, and anchor fixation in bone) may collectively contribute to gap formation at the tendon bone interface, and potentially, to failure of the mechanical construct. We speculate that this may be especially concerning in elderly patients who not only are predisposed to osteopenic bone, but also have poor soft-tissue quality, decreased vascular supply and arguably poorer healing potential.20
Clinically, if a knotless anchor is to be used for a rotator cuff repair in osteopenic bone, an anchor with the sutures completely internal to the anchor body should be considered. This is particularly relevant if the surgeon performs a single row repair, as cyclic loading stress from the rotator cuff tendon is transferred directly to the suture and anchor, as we simulated in this study. However, if the knotless anchor is to be used as a lateral row fixation device as part of a double row construct, the effect of suture cutting through bone may be less concerning. In these constructs, the load would be predominantly focused on the medial anchors (especially if the medial sutures are tied), and the load on the lateral knotless anchors and sutures may be minimal.21,22 For younger patients with healthy bone, the effect of suture cutting through bone should be lessened. However, surgeons should still be aware of the possible adverse effect as bone quality can be locally inconsistent, even in ‘healthy’ bone.23
There are number of limitations in our study. First, this is a biomechanical study where the anchors were tested in cadaveric bones and foam blocks, and therefore may not necessarily represent in vivo conditions. However, we aimed to isolate the effects of suture cutting through bone from other multiple factors involved in the clinical situation after a rotator cuff repair, which may not be practical in in vivo or clinical studies. Comparative clinical studies evaluating different knotless anchor designs are necessary to establish whether suture handling is associated with fixation failure. Secondly, the mechanical testing was performed using a suture loop rather than a tendon construct. While this may be considered a ‘worse-case’ scenario, we chose this design to isolate the factors related to the anchor and sutures, particularly the effect of ‘suture cutting through bone’. In vivo, other factors related to the tendon factor (e.g. tendon strain, suture hole widening, suture cutting through tendon) may affect the overall result. Thirdly, while we chose MultiFIX P and SpeedScrew as representatives of two knotless suture anchor types, there are many other knotless suture anchors with variable features. Other different anchor properties, such as size, shape and suture locking mechanism, may additionally affect the results. However, in the current study, the suture loop was pulled in-line with the rotator cuff (approximately 60°) in order to isolate ‘suture cutting though bone’ because this angle permits oblique contact between the suture and the bone. We believe the two anchor types tested in our study represent internal and external knotless suture anchors and the principles and results are still valid. Lastly, although we tested anchors in cadaveric humeral bone, no attempt was made to determine the overall bone quality. While we did randomly assign the anchor and location to the cadaveric specimens to minimise the effect of cadaveric bone quality, we did not perform any bone testing (e.g. bone densitometry). However, it has previously been shown that even within the same cadaveric humeri, local bone quality can be significantly different within the cadaveric sample23 and therefore overall bone densitometry measurements may be misleading. As previous studies have evaluated the mechanical performance of suture anchors tested in foam blocks representing osteopenic bone,16 we chose to validate the principle of the effect of osteopenia in a foam block model to provide a uniform reproducible testing apparatus.
In conclusion, knotless suture anchors with sutures external to the anchor body may be at risk of losing tendon and anchor fixation due to ‘suture cutting through bone’, particularly when combined with osteopenic bone. This may be clinically relevant if these types of anchors are used in elderly patients with poor bone quality, particularly when used as a single row construct.
Funding Statement
The authors would like to acknowledge the materials and technical assistance provided by ArthroCare through an ArthroCare Grant Panel Independent Research Grant (I. K. Y. Lo and G. M. Thornton) for this study.
ICMJE conflict of interest
I. K. Y. Lo is a consultant for Arthrex Inc. and Artho Care Corp.
References
1 Sher JS , UribeJW, PosadaA, MurphyBJ, ZlatkinMB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg [Am]1995;77-A:10-15.PubMed Google Scholar
2 Randelli P , SpennacchioP, RagoneV, ArrigoniP, CasellaA, CabitzaP. Complications associated with arthroscopic rotator cuff repair: a literature review. Musculoskelet Surg2012;96:9-16.CrossrefPubMed Google Scholar
3 Tashjian RZ , HollinsAM, KimHM, et al.. Factors affecting healing rates after arthroscopic double-row rotator cuff repair. Am J Sports Med2010;38:2435-2442.CrossrefPubMed Google Scholar
4 Randelli P , CucchiD, RagoneV, de GirolamoL, CabitzaP, RandelliM. History of rotator cuff surgery. Knee Surg Sports Traumatol Arthrosc2015;23:344-362.CrossrefPubMed Google Scholar
5 Thal R . A knotless suture anchor. Design, function, and biomechanical testing. Am J Sports Med2001;29:646-649.CrossrefPubMed Google Scholar
6 Barber FA , BavaED, SpencinerDB, PiccirilloJ. Cyclic biomechanical testing of biocomposite lateral row knotless anchors in a human cadaveric model. Arthroscopy2013;29:1012-1018.CrossrefPubMed Google Scholar
7 Pietschmann MF , FroehlichV, FicklschererA, WegenerB, JanssonV, MullerPE. Biomechanical testing of a new knotless suture anchor compared with established anchors for rotator cuff repair. J Shoulder Elbow Surg2008;17:642-646.CrossrefPubMed Google Scholar
8 Pietschmann MF , GülecyüzMF, FieselerS, et al.. Biomechanical stability of knotless suture anchors used in rotator cuff repair in healthy and osteopenic bone. Arthroscopy2010;26:1035-1044.CrossrefPubMed Google Scholar
9 Robbe R , PalettaGA. Knotless suture-based anchors. Oper Tech Sports Med2004;12:221-224. Google Scholar
10 Leedle BP , MillerMD. Pullout strength of knotless suture anchors. Arthroscopy2005;21:81-85.CrossrefPubMed Google Scholar
11 Woodmass JM , MatthewsonG, OnoY, et al.. Suture locking of isolated internal locking knotless suture anchors is not affected by bone quality. Open Access J Sports Med2015;6:201-208. Google Scholar
12 Burkhart SS . Reprint of: The deadman theory of suture anchors: observations along a south Texas fence line. Arthroscopy2014;30:895-899.CrossrefPubMed Google Scholar
13 Barber FA , HapaO, BynumJA. Comparative testing by cyclic loading of rotator cuff suture anchors containing multiple high-strength sutures. Arthroscopy2010;26(Suppl):S134-S141.CrossrefPubMed Google Scholar
14 Lo IK , BurkhartSS, ChanKC, AthanasiouK. Arthroscopic knots: determining the optimal balance of loop security and knot security. Arthroscopy2004;20:489-502.CrossrefPubMed Google Scholar
15 Meyer DC , MayerJ, WeberU, MuellerA, KochPP, GerberC. Ultrasonically implanted PLA suture anchors are stable in osteopenic bone. Clin Orthop Relat Res2006;442:143-148.CrossrefPubMed Google Scholar
16 Poukalova M , YakackiCM, GuldbergRE, et al.. Pullout strength of suture anchors: effect of mechanical properties of trabecular bone. J Biomech2010;43:1138-1145.CrossrefPubMed Google Scholar
17 Tingart MJ , AprelevaM, LehtinenJ, ZurakowskiD, WarnerJJ. Anchor design and bone mineral density affect the pull-out strength of suture anchors in rotator cuff repair: which anchors are best to use in patients with low bone quality?Am J Sports Med2004;32:1466-1473.CrossrefPubMed Google Scholar
18 Yakacki CM , PoukalovaM, GuldbergRE, et al.. The effect of the trabecular microstructure on the pullout strength of suture anchors. J Biomech2010;43:1953-1959.CrossrefPubMed Google Scholar
19 Burkhart SS , JohnsonTC, WirthMA, AthanasiouKA. Cyclic loading of transosseous rotator cuff repairs: tension overload as a possible cause of failure. Arthroscopy1997;13:172-176.CrossrefPubMed Google Scholar
20 Hattrup SJA . Rotator cuff repair: Relevance of patient age. J Shoulder Elbow Surg1995;4:95-100.CrossrefPubMed Google Scholar
21 Leek BT , RobertsonC, MaharA, PedowitzRA. Comparison of mechanical stability in double-row rotator cuff repairs between a knotless transtendon construct versus the addition of medial knots. Arthroscopy2010;26(Suppl):S127-S133.CrossrefPubMed Google Scholar
22 Mall NA , LeeAS, ChahalJ, et al.. Transosseous-equivalent rotator cuff repair: a systematic review on the biomechanical importance of tying the medial row. Arthroscopy2013;29:377-386.CrossrefPubMed Google Scholar
23 Kirchhoff C , BraunsteinV, MilzS, et al.. Assessment of bone quality within the tuberosities of the osteoporotic humeral head: relevance for anchor positioning in rotator cuff repair. Am J Sports Med2010;38:564-569.CrossrefPubMed Google Scholar
