




Abstract
Objectives
Our study aimed to examine not only the incidence but also the impact of noise from two types of total hip replacement articulations: ceramic-on-ceramic and ceramic-on-polyethylene.
Methods
We performed a case-controlled study comparing subjective and objective questionnaire scores of patients receiving a ceramic-on-ceramic or a ceramic-on-polyethylene total hip replacement by a single surgeon.
Results
There was a threefold higher incidence of noise from patients in the ceramic-on-ceramic group compared with the control group. The impact of this noise was significant for patients both subjectively and objectively.
Conclusions
This study reports a high patient impact of noise from ceramic-on-ceramic total hip replacements. This has led to a change in practice by the principal author.
Cite this article: Bone Joint Res 2014;3:183–6.
Article focus
To investigate the incidence and impact of noise from ceramic-on-ceramic compared with ceramic-on-polyethylene total hip replacements.
Key messages
Noise from ceramic-on-ceramic total hip replacements is not only more common than in ceramic-on-polyethylene articulations, but it is also particularly troublesome for the patient.
Strengths and limitations
Strengths: This study is a single-surgeon series and 179 patients were evaluated.
We used a validated questionnaire method.
Limitation: There is very little data published on this issue.
Introduction
Total hip replacement (THR) has evolved with the improved application of tribological technology. Polyethylene wear and osteolysis, leading to early aseptic loosening in young active patients, has been prolific in the rise in interest in ceramic bearings. Ceramic bearings are smooth, hard, scratch-resistant, have high wettability and very low rates of wear, and excellent survivorship which has been observed with their use.1,2 However, concern remains over ceramic fracture and squeaking.
Squeaking and noise from ceramic bearing THRs is well recognised, with a reported incidence of 0% to 35%.3-6 The precise aetiology is unknown, but is believed to be multifactorial. The likely culprits include component design and combination,4,7 cup malposition,5 abnormal wear pattern, patient weight, soft-tissue crepitus and insert versus shell movement.8 Therefore, squeaking is not merely a nuisance but may indicate an insidious biomechanical problem.
Given the potentially serious biomechanical causes of squeaking, there have been numerous studies in this area, but few have examined the direct impact of this intriguing phenomenon on the patient. The aim of this study was to discern the impact of such noise on the patient’s quality of life.
Patients and Methods
We identified 112 patients from hospital records of theatre lists who had received 36 mm ceramic-on-ceramic (CoC) THRs, and compared them with 159 patient controls who had received a 28 mm ceramic-on-polyethylene (CoP) component within two years of this study. We used the New Zealand Joint Registry to identify an age-matched control group from the senior author’s practice (GH). All patients had identical cemented femoral components (Zimmer, Warsaw, Indiana) and either Mathys (Bettlach, Switzerland) classic polyethylene cups or Mathys SeleXys uncemented cup, which were inserted through a posterior approach. All operations were performed by the senior author (JGH).
Patients were invited to participate, and received a specific validated questionnaire by post for both subjective and objective assessments (Fig. 1).
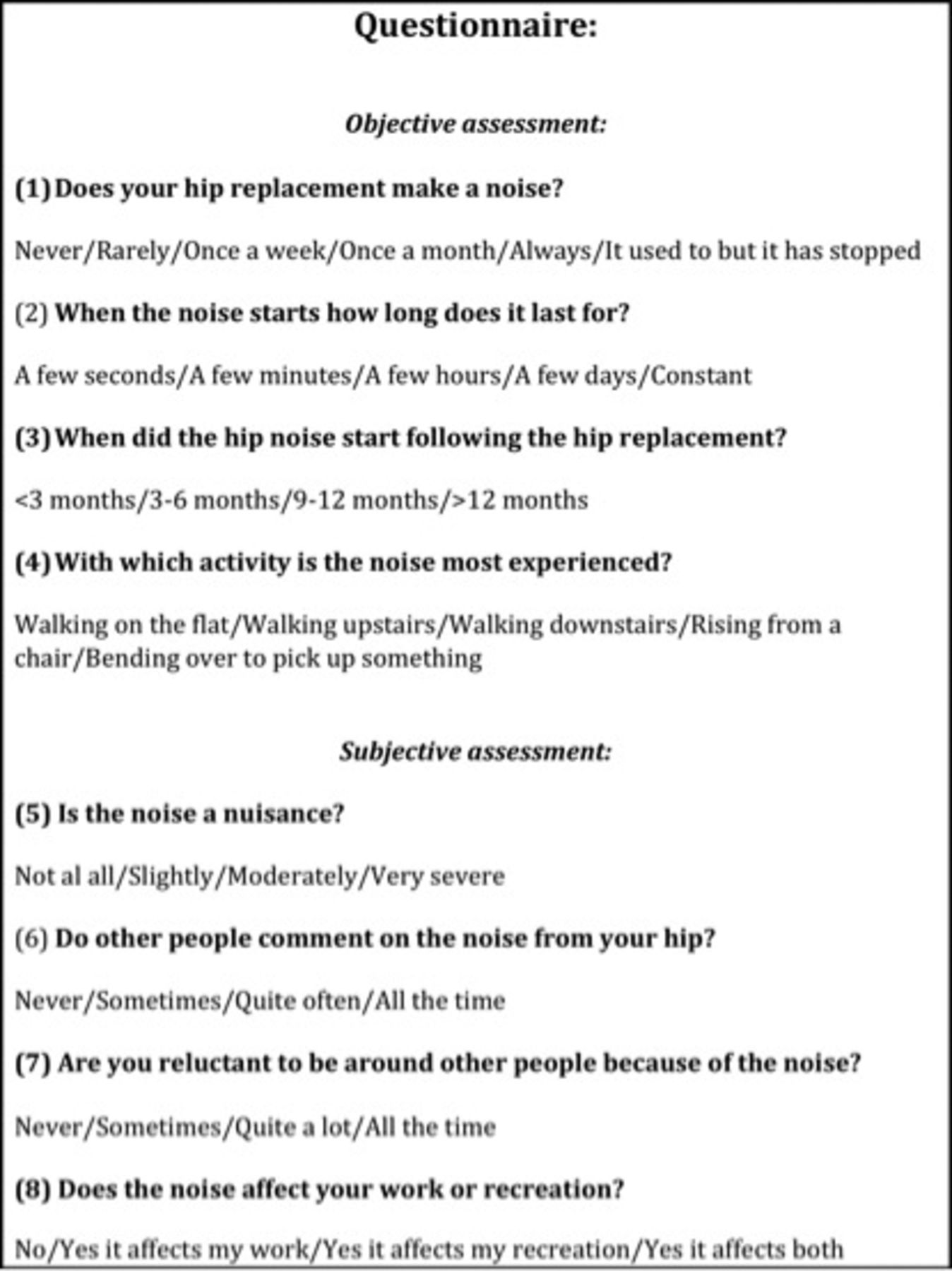
Fig. 1
Questionnaire for assessment of subjective and objective impact of noise.
Statistical analysis
Results were compared between the study and control groups using the chi-square or Mann–Whitney U tests.
Results
The response rate was 61.6% in the study group (69/112) and 69.2% in the control group (110/159).
Subjective assessment
Overall, we found that 37.7% (26/69) of CoC THRs reported noise compared with 12.7% (14/110) of the control CoP group, which is significant (p < 0.001). In addition, the patients within the control group were significantly more likely never to report any noise, while the study group were significantly more likely always to perceive noise (p < 0.001) (Fig. 2) of CoC THRs reported noise compared with 12.7% (14/110) of the control CoP group, which is significant (p < 0.001). In addition, the patients within the control group were significantly more likely never to report any noise, while the study group were significantly more likely always to perceive noise (p < 0.001) (Fig. 2) of the control CoP group, which is significant (p < 0.001). In addition, the patients within the control group were significantly more likely never to report any noise, while the study group were significantly more likely always to perceive noise (p < 0.001) (Fig. 2). In addition, the patients within the control group were significantly more likely never to report any noise, while the study group were significantly more likely always to perceive noise (p < 0.001) (Fig. 2) (Fig. 2). Patients in the study group were significantly more likely to have constant noise compared with the control group (p < 0.01) (Fig. 3) (Fig. 3). There were no significant differences in the incidence of shorter noise occurrences between groups. CoC patients were significantly more likely to report noise after a year compared with controls (p < 0.01) (Fig. 4) (Fig. 4) whereas the timing of noise commencing prior to one year following surgery was similar in both groups. Patients with a CoC THR tended to notice noise significantly more when bending over (Fig. 5) (p < 0.01). Other physical activities did not discriminate between groups in terms of noise perceived.
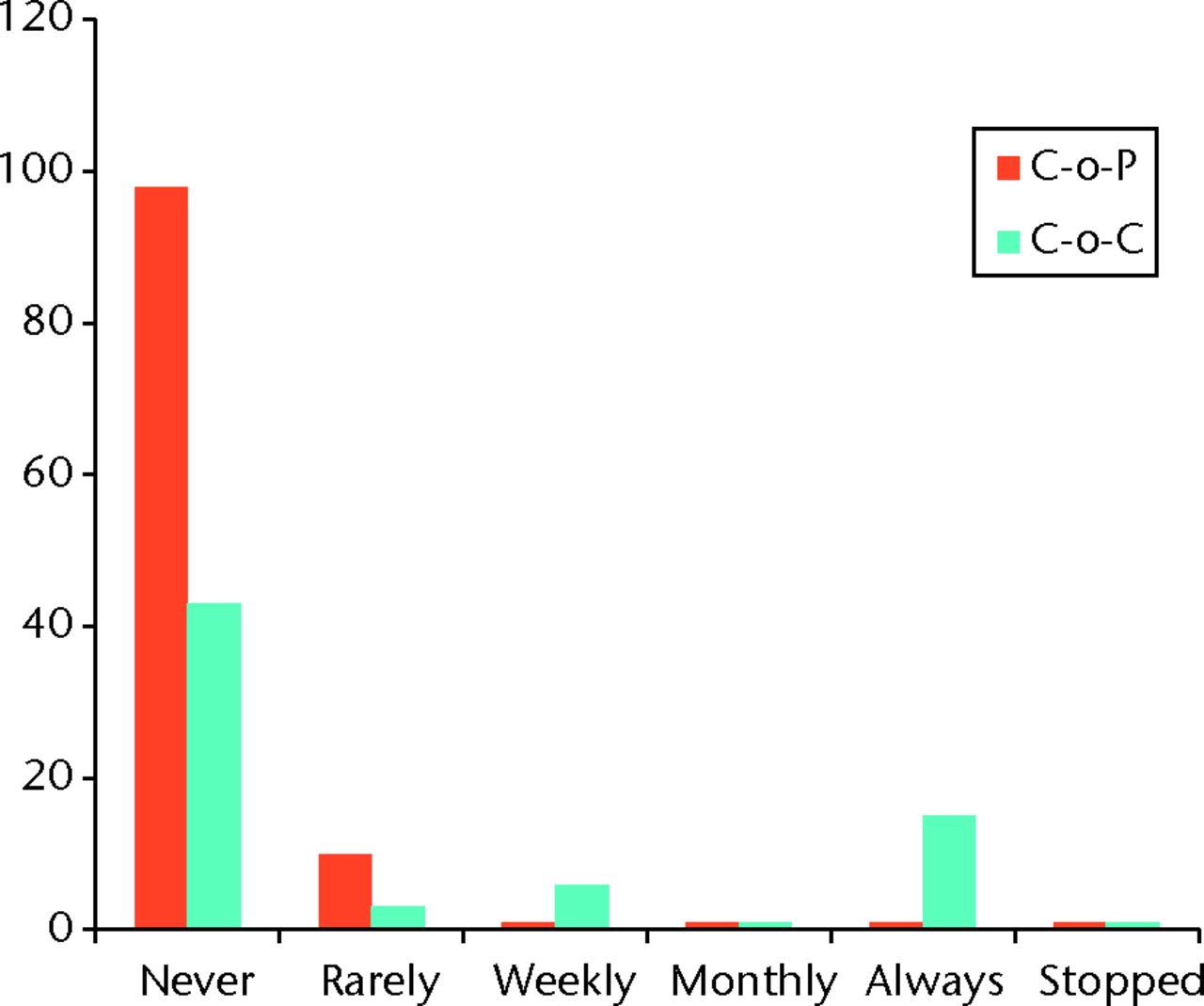
Fig. 2
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘Does your hip make a noise?’
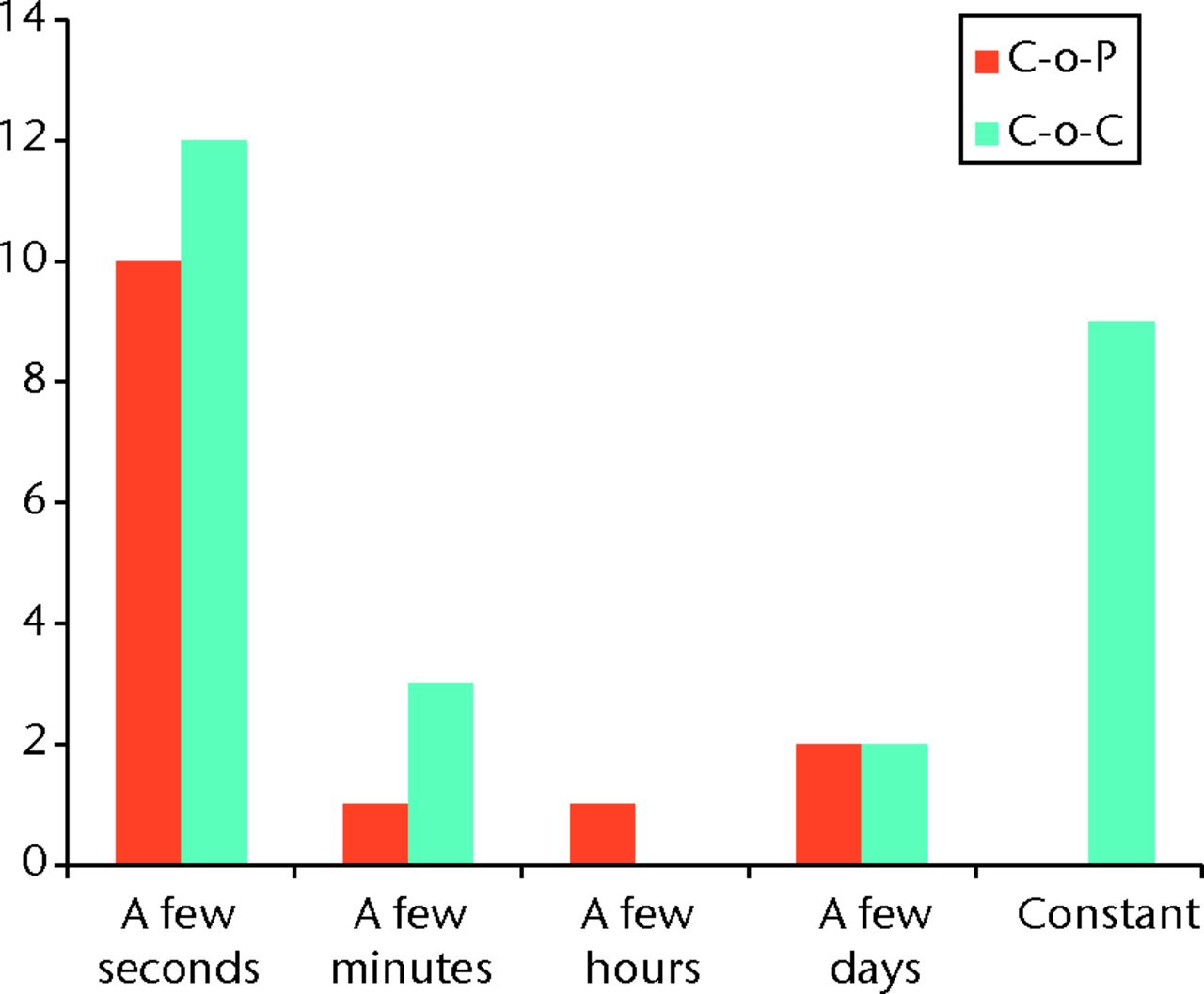
Fig. 3
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question 'How long does the noise last?'
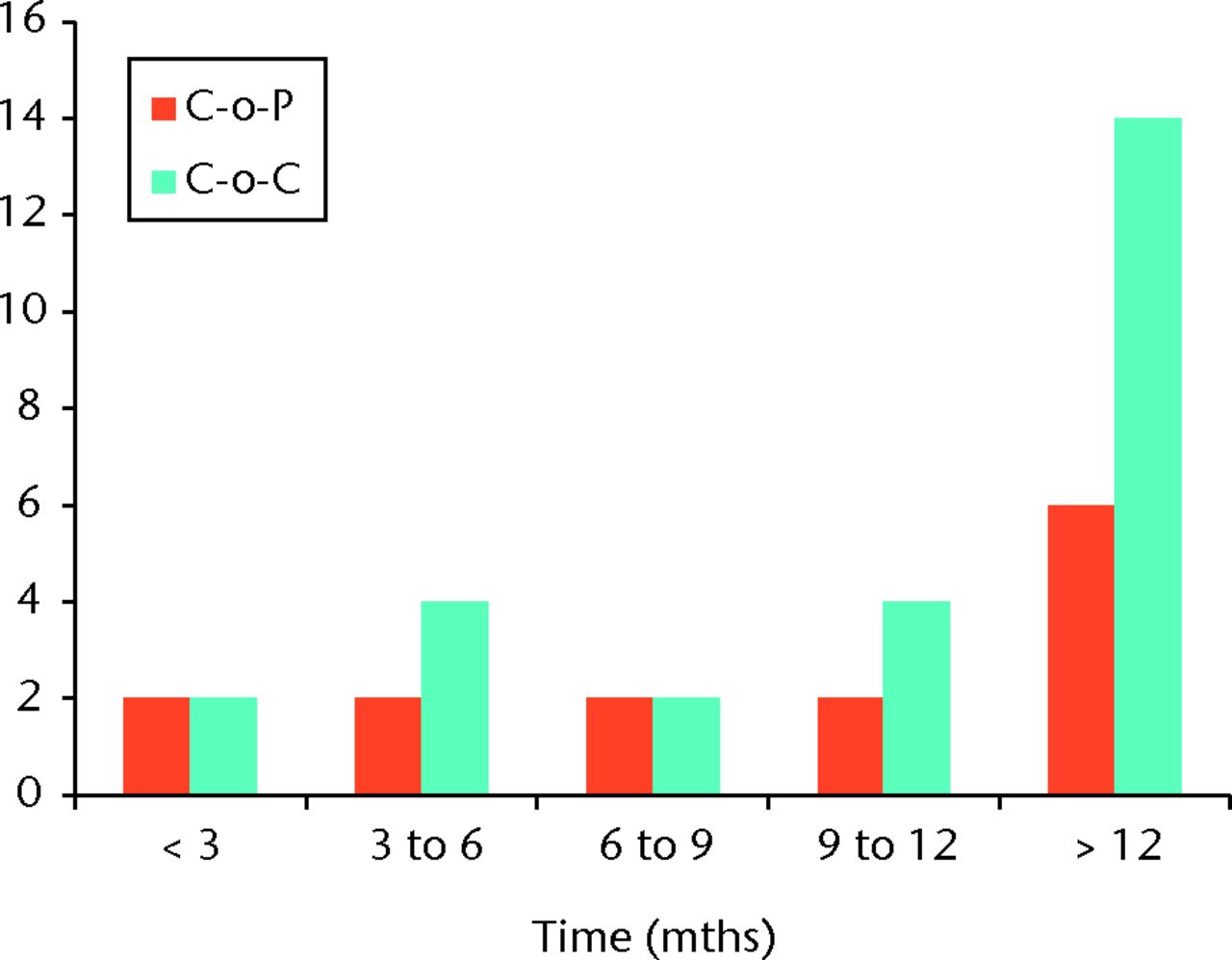
Fig. 4
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘When did the noise start?’
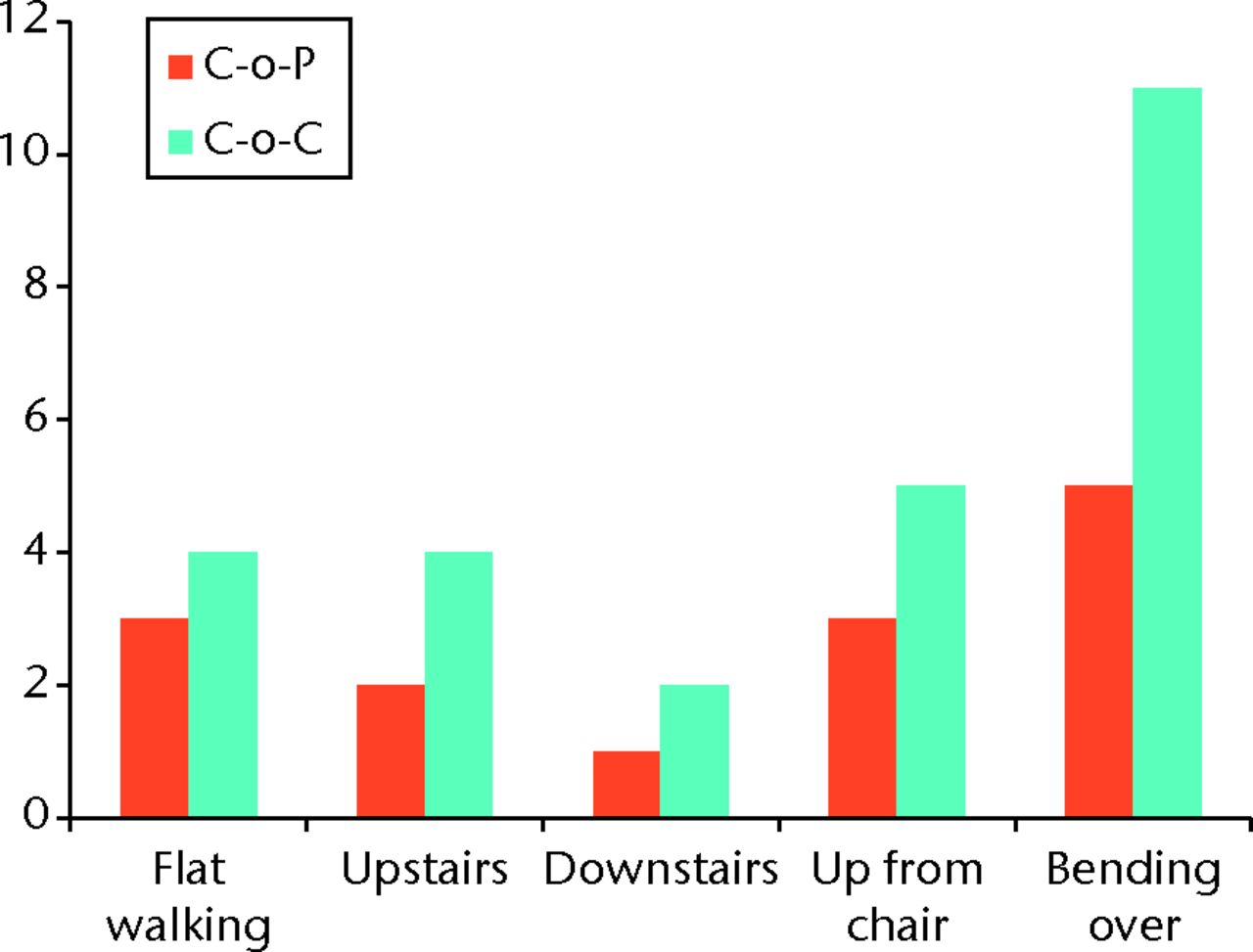
Fig. 5
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘What activity brings about the noise?’
Objective assessment
The noise experienced by patients in the study group generally tended to be more troublesome and remarked upon more by other people than was the noise experienced in the control group, the latter significantly so (p < 0.01) (Figs 6 and 7). The noise from patients with a CoC THR tended to be more embarrassing to those patients than noise experienced by patients from the control group (Fig. 8) (Figs 6 and 7). The noise from patients with a CoC THR tended to be more embarrassing to those patients than noise experienced by patients from the control group (Fig. 8). The noise from patients with a CoC THR tended to be more embarrassing to those patients than noise experienced by patients from the control group (Fig. 8). The noise in both groups did not tend to be restrictive on work or recreational activity in the majority of patients, however, any restriction that was encountered tended to be in those with a CoC THR (p < 0.01) (Fig. 9) (Fig. 9).
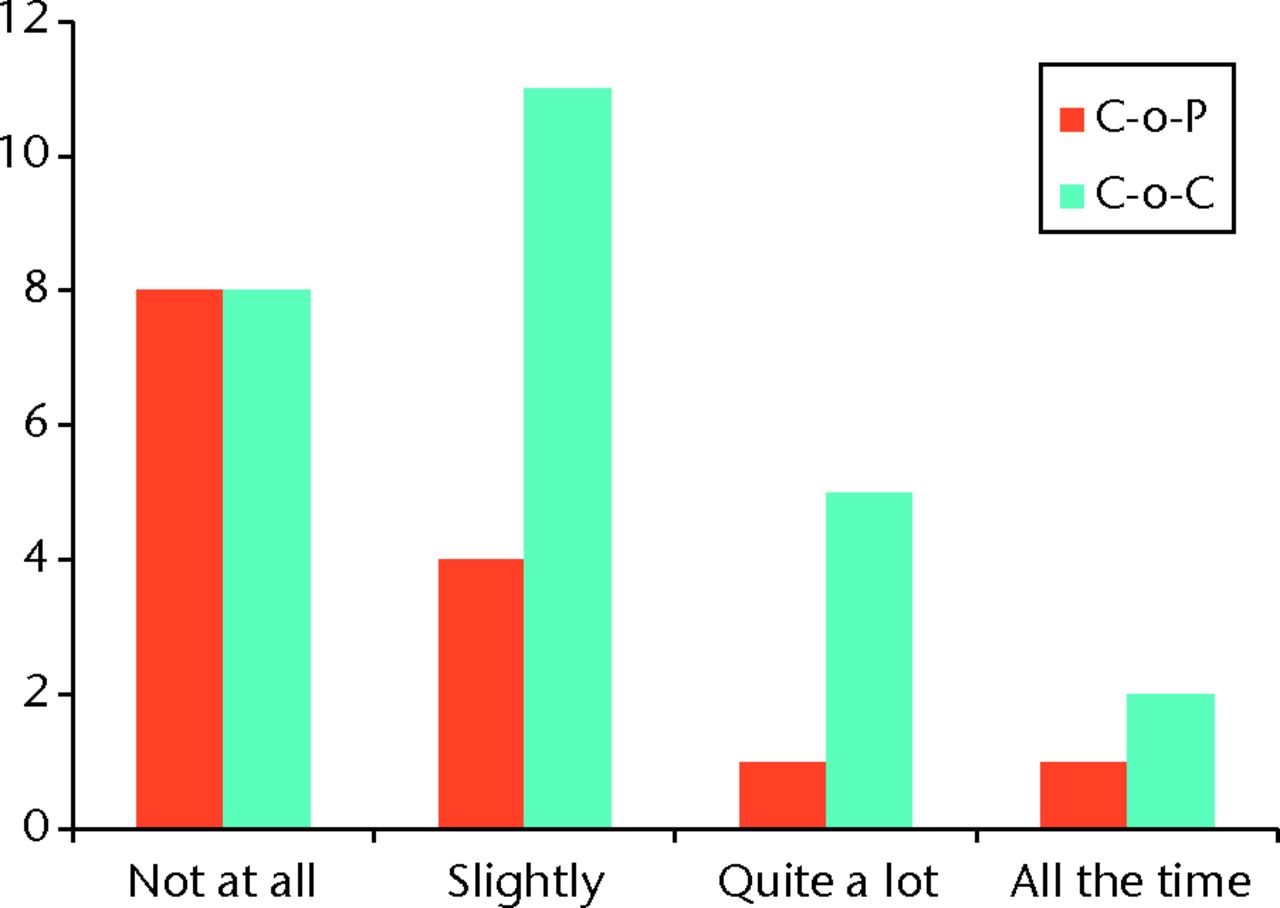
Fig. 6
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘Is the noise a nuisance?’
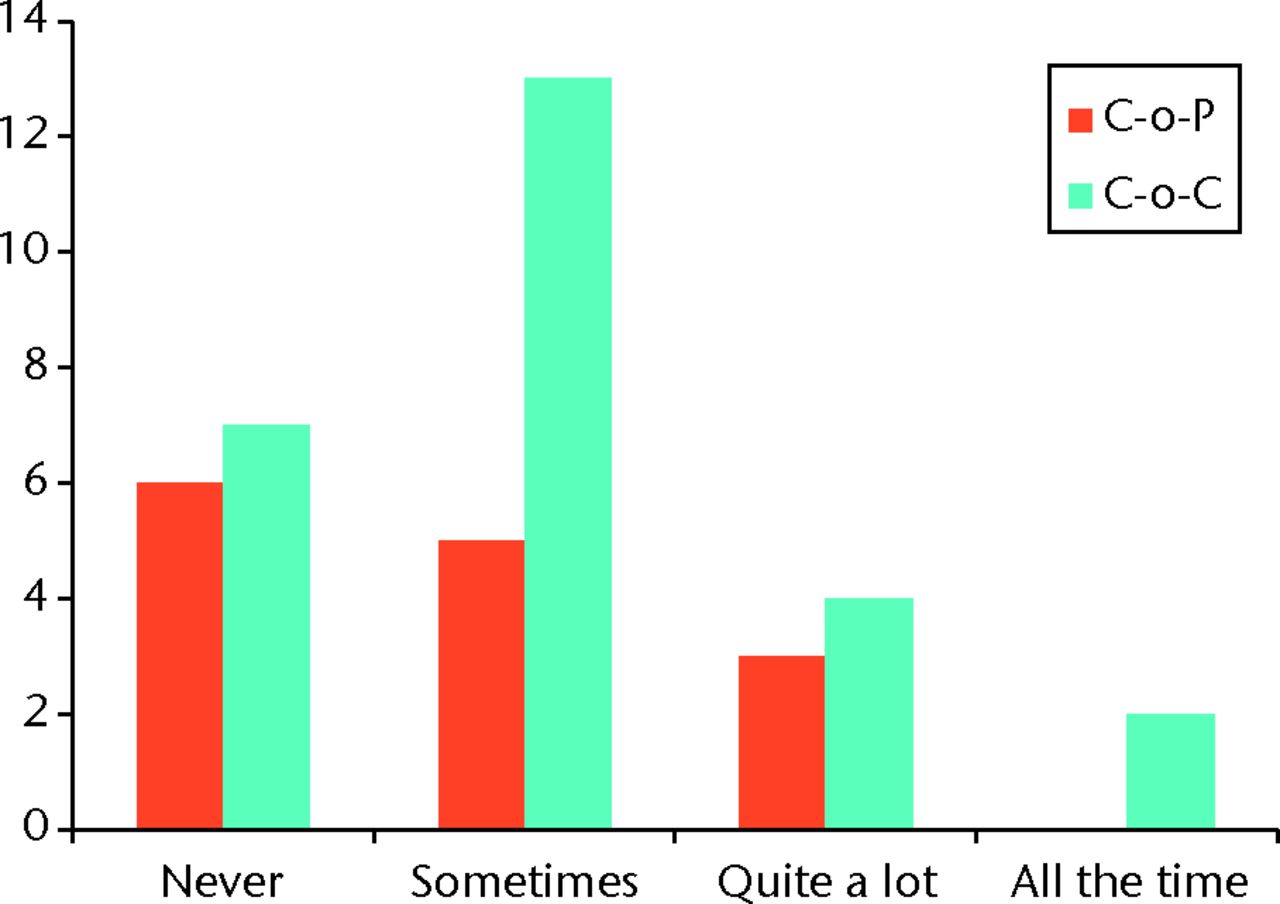
Fig. 7
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘Do other people comment?’
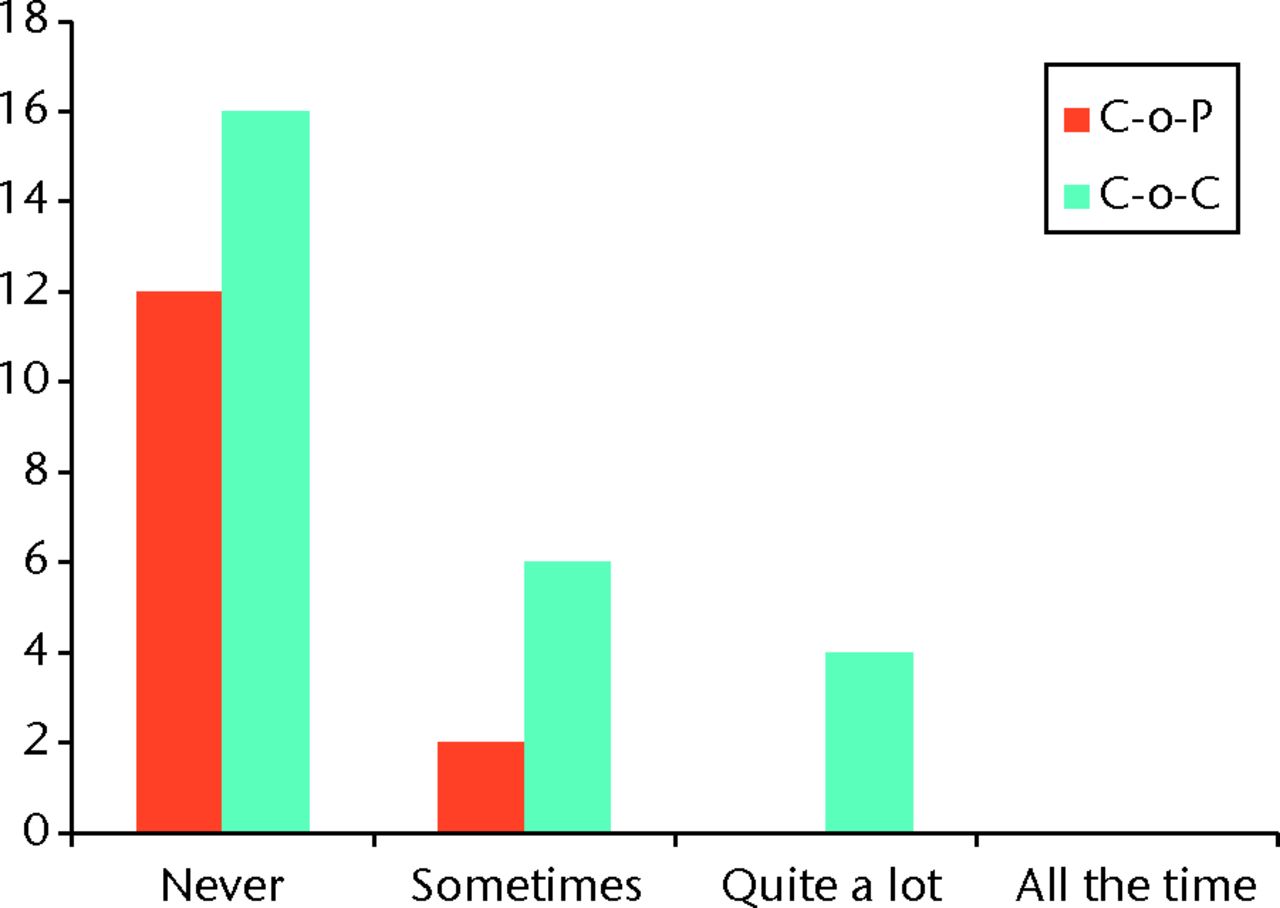
Fig. 8
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘Are you reluctant to be around other people because of the noise?’
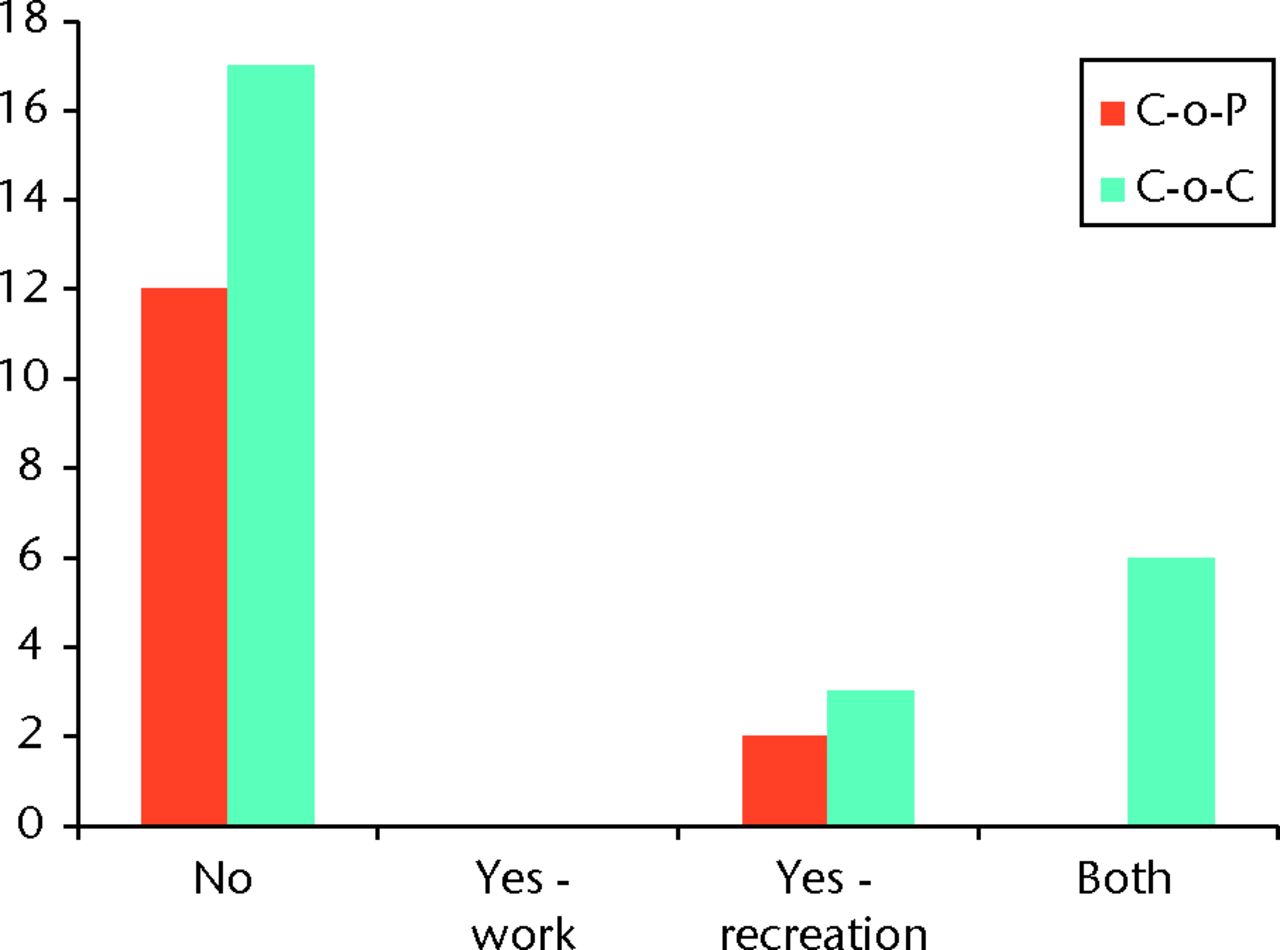
Fig. 9
Graph showing results of both ceramic-on-ceramic (CoC) and ceramic-on-polyethylene (CoP) groups for the question ‘Does the noise affect your work or recreation?’
Discussion
In our study, noise emanating from CoC bearing THRs was more than three times more common than from CoP. Furthermore, this noise has a significant impact on patients both subjectively and objectively. In another series of 306 patients (336 CoC hips) the incidence of noise was 17%, and 92% were otherwise symptom free.9 The findings from our study were more striking given a 37% incidence and greater reported symptoms.
Squeaking after CoC THR has been characterised by Sariali et al.10 Interestingly, two distinct noise frequencies were observed: one at 2.4 kHz when walking and the other at 1.4 kHz when rising from a flexed position. In vitro simulation showed that a third boy particle produced a sound similar to that observed in the walking squeakers. It may be that the lower frequency sound in rising from a chair was more troublesome for our patient group.
In a prospective multicentre trial comparing CoC or CoP bearing combinations, there was no significant difference in clinical outcome scores or revision rates between the two groups, yet there was much less linear wear in the first group. However, the CoC group had a 3% incidence of audible noise and a 2.6% ceramic fracture risk.11 Following this study, the senior author (JGH) has dramatically reduced his use of CoC bearings in THR: CoC bearings are now only used by the senior author (JGH) if the patient makes a specific request after an appropriate discussion.
Acknowledgements: The authors thank the New Zealand National Joint Registry for the provision of age-matched control groups.
1 Lee YK , HaYC, YooJJ, et al.Alumina-on-alumina total hip arthroplasty: a concise follow-up, at a minimum of ten years, of a previous report. J Bone Joint Surg [Am]2010;92-A:1715–1719.CrossrefPubMed Google Scholar
2 Hernigou P , ZilberS, FilippiniP, PoignardA. Ceramic-ceramic bearing decreases osteolysis: a 20-year study versus ceramic-polyethylene on the contralateral hip. Clin Orthop Relat Res2009;467:2274–2280.CrossrefPubMed Google Scholar
3 Cogan A , NizardR, SedelL. Occurrence of noise in alumina-on-alumina total hip arthroplasty. A survey on 284 consecutive hips. Orthop Traumatol Surg Res2011;97:206–210.CrossrefPubMed Google Scholar
4 Parvizi J , AdeliB, WongJC, RestrepoC, RothmanRH. A squeaky reputation: the problem may be design-dependent. Clin Orthop Relat Res2011;469:1598–1605.CrossrefPubMed Google Scholar
5 Sexton SA , YeungE, JacksonMP, et al.The role of patient factors and implant position in squeaking of ceramic-on-ceramic total hip replacements. J Bone Joint Surg [Br]2011;93-B:439–442.CrossrefPubMed Google Scholar
6 Swanson TV , PetersonDJ, SeethalaR, BlissRL, SpellmonCA. Influence of prosthetic design on squeaking after ceramic-on-ceramic total hip arthroplasty. J Arthroplasty2010;25(6Suppl):36–42.CrossrefPubMed Google Scholar
7 Restrepo C , PostZD, KaiB, HozackWJ. The effect of stem design on the prevalence of squeaking following ceramic-on-ceramic bearing total hip arthroplasty. J Bone Joint Surg [Am]2010;92-A:550–557.CrossrefPubMed Google Scholar
8 Imbuldeniya AM , PearceSJ, WalterWL, ZicatBA, WalterWK. Squeaking: Current knowledge and how to avoid it. Curr Rev Musculoskelet Med2013;6:342–349.CrossrefPubMed Google Scholar
9 Mai K , VeriotiC, EzzetKA, et al.Incidence of 'squeaking' after ceramic-on-ceramic total hip arthroplasty. Clin Orthop Relat Res2010;468:413–417.CrossrefPubMed Google Scholar
10 Sariali E , JinZ, StewartT, FisherJ. Spectral characterization of squeaking in ceramic-on-ceramic total hip arthroplasty: comparison of in vitro and in vivo values. J Orthop Res2012;30:185–189.CrossrefPubMed Google Scholar
11 Amanatullah DF , LandaJ, StraussEJ, et al.Comparison of surgical outcomes and implant wear between ceramic-ceramic and ceramic-polyethylene articulations in total hip arthroplasty. J Arthroplasty2011;26(6Suppl):72–77.CrossrefPubMed Google Scholar
Funding statement:
None declared
Author contributions:
M. C. Wyatt: Data analysis, Writing the paper
S. Jesani: Data collection
C. Frampton: Data analysis
P. Devane: Writing the paper
J. G. Horne: Writing the paper
ICMJE Conflict of Interest:
None declared
©2014 The British Editorial Society of Bone & Joint Surgery. This is an open-access article distributed under the terms of the Creative Commons Attributions licence, which permits unrestricted use, distribution, and reproduction in any medium, but not for commercial gain, provided the original author and source are credited.
