




Abstract
Aims
There are concerns regarding nail/medullary canal mismatch and initial stability after cephalomedullary nailing in unstable pertrochanteric fractures. This study aimed to investigate the effect of an additional anteroposterior blocking screw on fixation stability in unstable pertrochanteric fracture models with a nail/medullary canal mismatch after short cephalomedullary nail (CMN) fixation.
Methods
Eight finite element models (FEMs), comprising four different femoral diameters, with and without blocking screws, were constructed, and unstable intertrochanteric fractures fixed with short CMNs were reproduced in all FEMs. Micromotions of distal shaft fragment related to proximal fragment, and stress concentrations at the nail construct were measured.
Results
Micromotions in FEMs without a blocking screw significantly increased as nail/medullary canal mismatch increased, but were similar between FEMs with a blocking screw regardless of mismatch. Stress concentration at the nail construct was observed at the junction of the nail body and lag screw in all FEMs, and increased as nail/medullary canal mismatch increased, regardless of blocking screws. Mean stresses over regions of interest in FEMs with a blocking screw were much lower than regions of interest in those without. Mean stresses in FEMs with a blocking screw were lower than the yield strength, yet mean stresses in FEMs without blocking screws having 8 mm and 10 mm mismatch exceeded the yield strength. All mean stresses at distal locking screws were less than the yield strength.
Conclusion
Using an additional anteroposterior blocking screw may be a simple and effective method to enhance fixation stability in unstable pertrochanteric fractures with a large nail/medullary canal mismatch due to osteoporosis.
Cite this article: Bone Joint Res 2022;11(3):152–161.
Article focus
-
To investigate the effect of an additional anteroposterior (AP) blocking screw on the bone-nail construct for nail/medullary canal mismatch after short cephalomedullary nailing in unstable pertrochanteric fractures.
Key messages
-
The mean stresses at the nail construct and micromotions of distal shaft fragment related to proximal fragment significantly increase as the nail/medullary canal mismatch increases in specific unstable pertrochanteric fracture models fixed with a short cephalomedullary nail.
-
Using an additional AP blocking screw for these fractures with nail/medullary canal mismatch greatly reduces micromotions of distal shaft fragment and stress concentration at the nail construct.
-
The additional AP blocking screw can be a simple and effective method to enhance fixation stability in unstable pertrochanteric fractures with a large nail/medullary canal mismatch due to osteoporosis.
Strengths and limitations
-
This is the first finite element analysis to investigate the effect of an additional AP blocking screw on fixation instability due to nail/medullary canal mismatch after cephalomedullary nailing in specific unstable pertrochanteric fractures.
-
Large-cohort clinical comparative studies are needed to confirm our results, and to verify the availability of a blocking screw in these fractures, as the current findings are based on an experimental study.
Introduction
Pertrochanteric hip fracture is one of the most common injuries in the elderly population, and its incidence is continuously increasing owing to demographic changes and the increased incidence of osteoporosis.1,2 Short cephalomedullary nails (CMNs) have been widely used for unstable pertrochanteric fractures, including reverse obliquity, subtrochanteric extension, and fracture extension into the lateral wall, as they are biomechanically superior to extramedullary devices and are less invasive.3 In addition to the continuous improvements in implant design to enhance fixation stability, short CMNs have showed favourable outcomes for the aforementioned fractures.4
As the ageing population increases, the number of elderly patients who suffer unstable pertrochanteric fractures with marked osteoporosis and the corresponding risk of fixation failure in this population increases.5 In osteoporotic elderly patients, the medullary canal diameter widens, whereas the cortex becomes thinner,6 and the variety of usable short CMN diameters is limited in practical terms due to stock issues (although this may be slightly different for each manufacturer). Therefore, a nail/medullary canal mismatch may occur after cephalomedullary nailing in osteoporotic pertrochanteric fractures, especially at the metaphyseal-diaphyseal junction. The distal shaft fragment may move mediolaterally along the axis of a distal locking screw when a large nail/medullary canal mismatch with no nail-cortex contact occurs,7 consequently causing fixation instability intraoperatively or postoperatively in specific unstable fracture patterns, and possibly increasing the risk of nonunion, fixation failure, or peri-implant fracture. Although it has not been addressed in the literature yet, and various treatment options can be considered, using an additional anteroposterior (AP) blocking screw in such a mismatch can be a simple and useful alternative to achieve more secure fixation without nail exchange. An additional AP blocking screw inserted adjacent to the nail, which is used when nailing in supra- or infraisthmic long bone fractures, reduces the width of the medullary canal and increases the mechanical stability of the bone-nail construct.8 This blocking screw can enhance fixation stability of the distal shaft fragment for nail/medullary canal mismatch after short cephalomedullary nailing in specific unstable pertrochanteric fracture patterns. However, there is little information on the effect of additional AP blocking screws on this mismatch after short cephalomedullary nailing in unstable pertrochanteric fractures.
Therefore, this finite element analysis (FEA) study aimed to mechanically investigate the effect of an additional AP blocking screw on the bone-nail construct for nail/medullary canal mismatch after short cephalomedullary nailing in unstable pertrochanteric fractures.
Methods
Finite element model
A previously verified 3D finite element model (FEM) was used in this study.9,10 We performed intact left femur CT at a transverse resolution of 1.0 mm in 1.0 mm increments. The geometry of the femur and medullary canal surfaces was reconstructed using CT slice images created using the Mimics program version 21.0 (Materialise, Belgium). The intact femoral shape was obtained through geometry extraction, and subsequently volume-meshed with isotropic tetrahedral element types. To verify FEM, a strain was measured by attaching a strain gauge at a total of 20 points on the anterior, posterior, medial, and lateral sides of the model, and compared with that of the study by Heiner and Brown.10 An osteoporotic bone model was reproduced according to a previously verified model.11 The unstable intertrochanteric fracture corresponding to AO/OTA 31-A3.3 was reproduced using the automatic solid and mesh generation program (ABAQUS) version 6.14 (Dassault Systems, France).12 The lesser trochanter was removed, and the fracture gap was set at 2 mm. To investigate the effectiveness of the blocking screw in varying degrees of nail/medullary canal mismatch, four FEMs with different medullary canal osteoporotic femur diameters – namely 16, 18, 20, and 22 mm – were implemented (Figure 1). Medullary canal diameter was measured at 10 cm below the mid lesser trochanter line, directly above the distal locking screw level.13
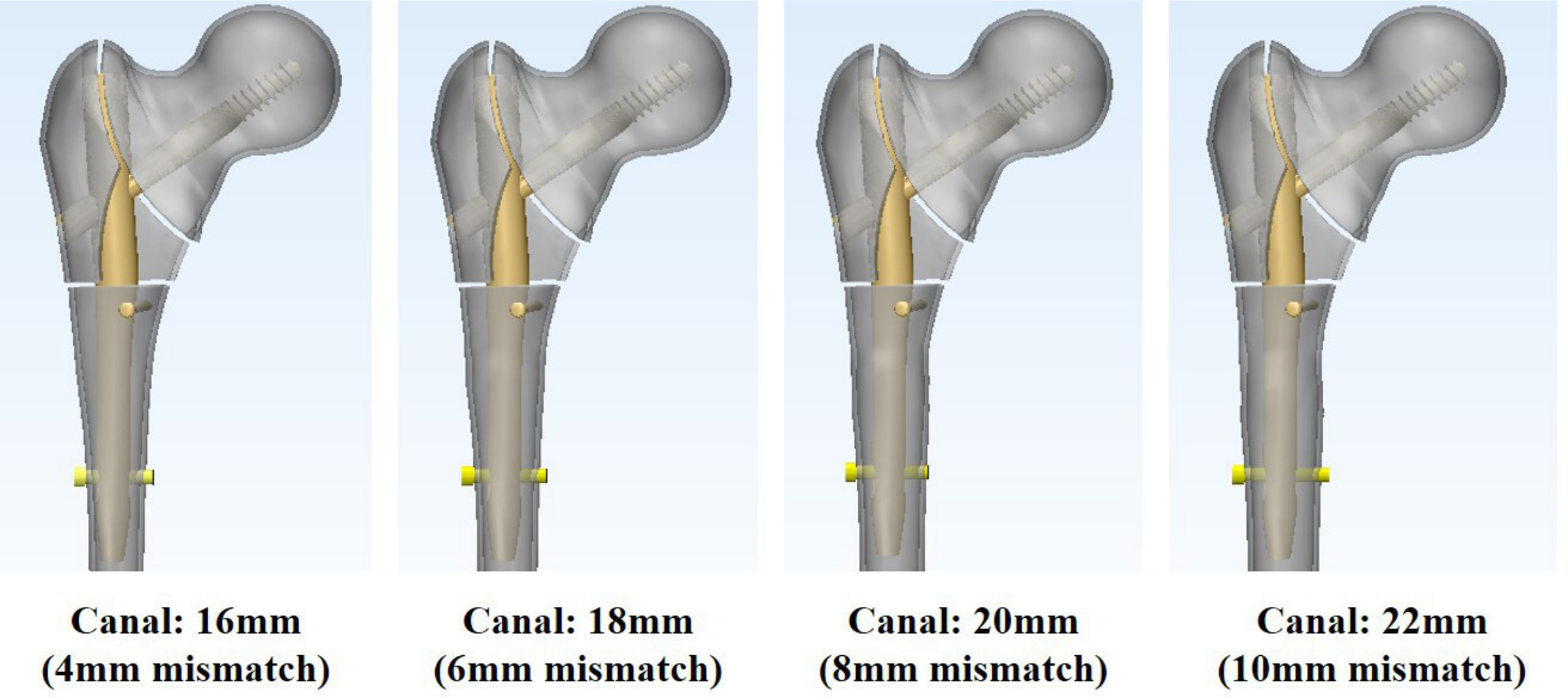
Fig. 1
Finite element models with different nail/medullary canal mismatch of unstable pertrochanteric fractures.
Short Gamma 3 CMNs (Stryker, USA), which were 170 mm in length and 12.0 mm in nail diameter, and had a 125° caput-collum-diaphyseal angle, a 100 mm lag screw length, and a 26 to 32 mm distal locking screw length, were used in this study. The geometry of all nail configurations was constructed in the intramedullary canal of each fractured FEM using ABAQUS. The lag screw was inserted into the centre-to-centre position in the femoral head, and the tip-apex distance was set to 22.92 mm on the AP and lateral views. Anatomical reduction was assumed in all models while maintaining the fracture gap. A cortical screw that was 32 mm in length and 3.5 mm in diameter was used as the blocking screw in the metaphyseal-diaphyseal junction, right inside the nail and at 10 mm below the transverse fracture line in the AP direction (Figure 1). Eight models were reproduced using combinations of four different medullary canal diameters, with and without blocking screws.
Eight-noded hexahedral and four-noded tetrahedral elements were created using ABAQUS to build the mesh of the fractured femur model and that of the Gamma 3 CMNs. These elements enabled the definition of the different material properties, and maintained contact conditions in the fracture plane.
Material properties
FEM analysis assumed that the bone structure has homogeneous and isotropic linear properties. The elastic modulus (E) was calculated using a mean CT Hounsfield unit (HU) value of 120.8 (standard deviation (SD) 41.8) to assign cancellous bone properties to the femoral model.14 The relationship between HU and elastic modulus was analyzed as follows:15,16
ρ = 13100 + 1067HU
E = 6850 ρ1.49
where ρ is the apparent density (g/cm3) and the unit of E is megapascal (MPa). The material properties of the femoral cortical bone, nail, and blocking screw were studied from earlier publications (Table I).17,18 For analytic purposes, titanium alloy (TI6Al4V) was used for the Gamma 3 nails (Young’s modulus 114 GPa, Poisson ratio 0.34), and stainless steel (316 L) was used for the blocking screws (Young’s modulus 147 GPa, Poisson ratio 0.29). Different material properties were assigned to different femoral regions.
Table I.
Material properties applied for the finite element model analysis.
| Variable | Elastic modulus (E), MPa | Poisson’s ratio (v) |
|---|---|---|
| Cortical bone | 17,000 | 0.3 |
| Cancellous bone | ||
| Normal bone | 920 | 0.2 |
| Osteoporotic bone | 574 | 0.2 |
| Cephalomedullary nail (TI6Al4V) | 113,800 | 0.34 |
| Blocking screw (316L) | 146,860 | 0.29 |
Boundary and loading conditions
Assuming the one-leg stance has normal ambulation, hip joint reaction forces (2,013.9 N, 300% of the body weight) were loaded on the femoral head, and an abductor muscle force (671.3 N, 100% of the body weight) was applied to the lateral surface of the greater trochanter.19,20 The forces of the hip joint reactions and abductor muscles were acting at a position 20° from the vertical line in the frontal plane (Figure 2). The general contact condition was applied using a friction coefficient of 0.42 to allow optimal movement between the nail and bone. The frictional coefficient was set at 0.2 for the nail and lag screw, 0.5 for the nail and blocking screw, and 0.46 for proximal and distal bone fragment interactions.21 A 'tie' contact condition was applied in this study, assuming full constraints between bone and bone, between bone and lag screw, and between bone and distal locking screw.
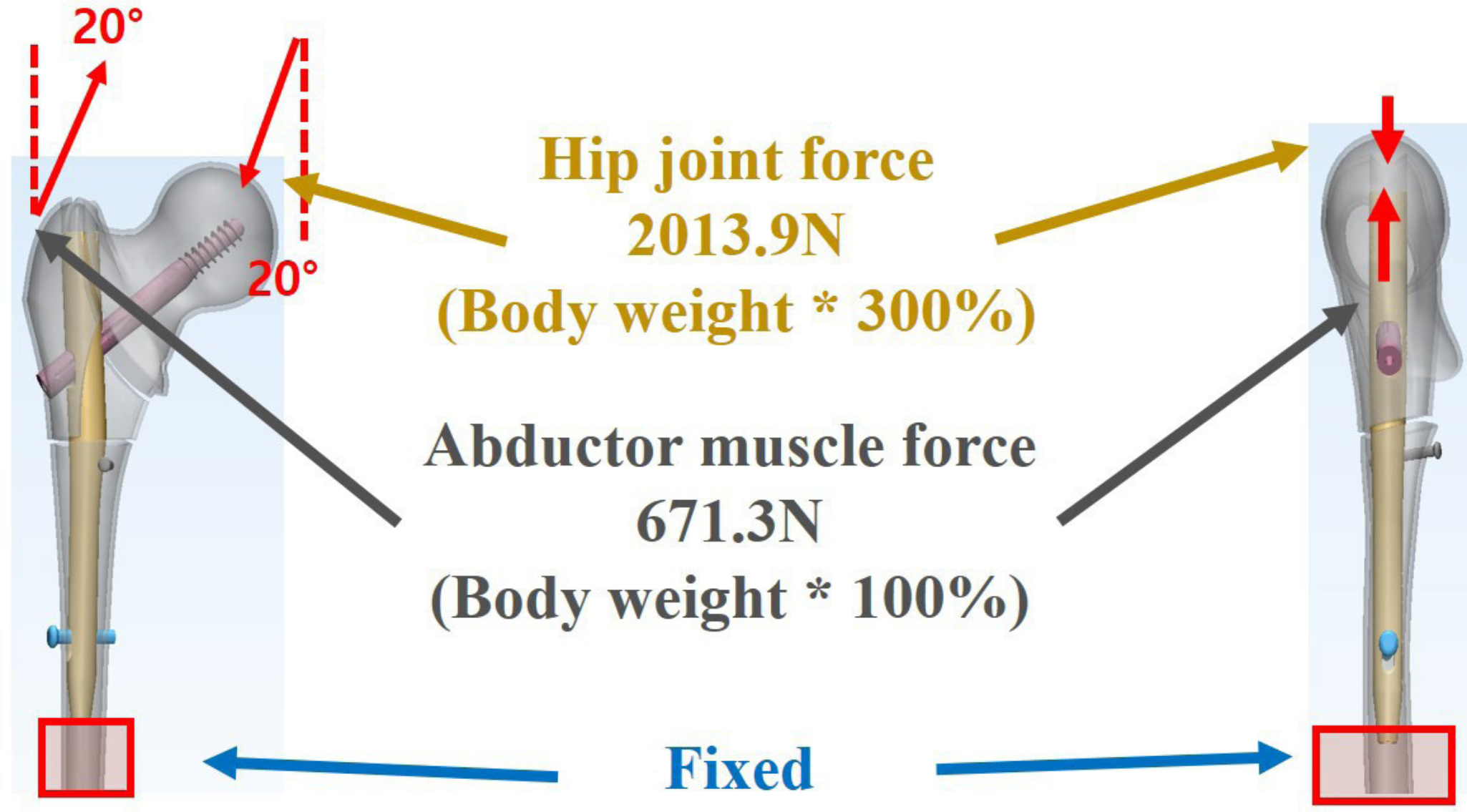
Fig. 2
Loading condition of the analysis model. Hip joint force, 2,013.9 N (body weight × 300%); abductor muscle force, 671.3 N (body weight × 100%).
FEM analysis
Eight FEMs were analyzed using combinations of four different nail/medullary canal mismatch – namely 4, 6, 8, and 10 mm – with or without blocking screws. The micromotion at the transverse fracture site around the metaphyseal-diaphyseal junction was measured to investigate distal shaft fragment mediolateral instability. Micromotion (μm) was defined as the distance between the positions of the distal fragment in the coronal plane before and after applying axial loading on each FEM. The micromotion of the distal fragment relative to the proximal fragment was measured through the mean coronal displacement of all nodes on the fracture surface between the proximal and distal fragments (Figure 3).
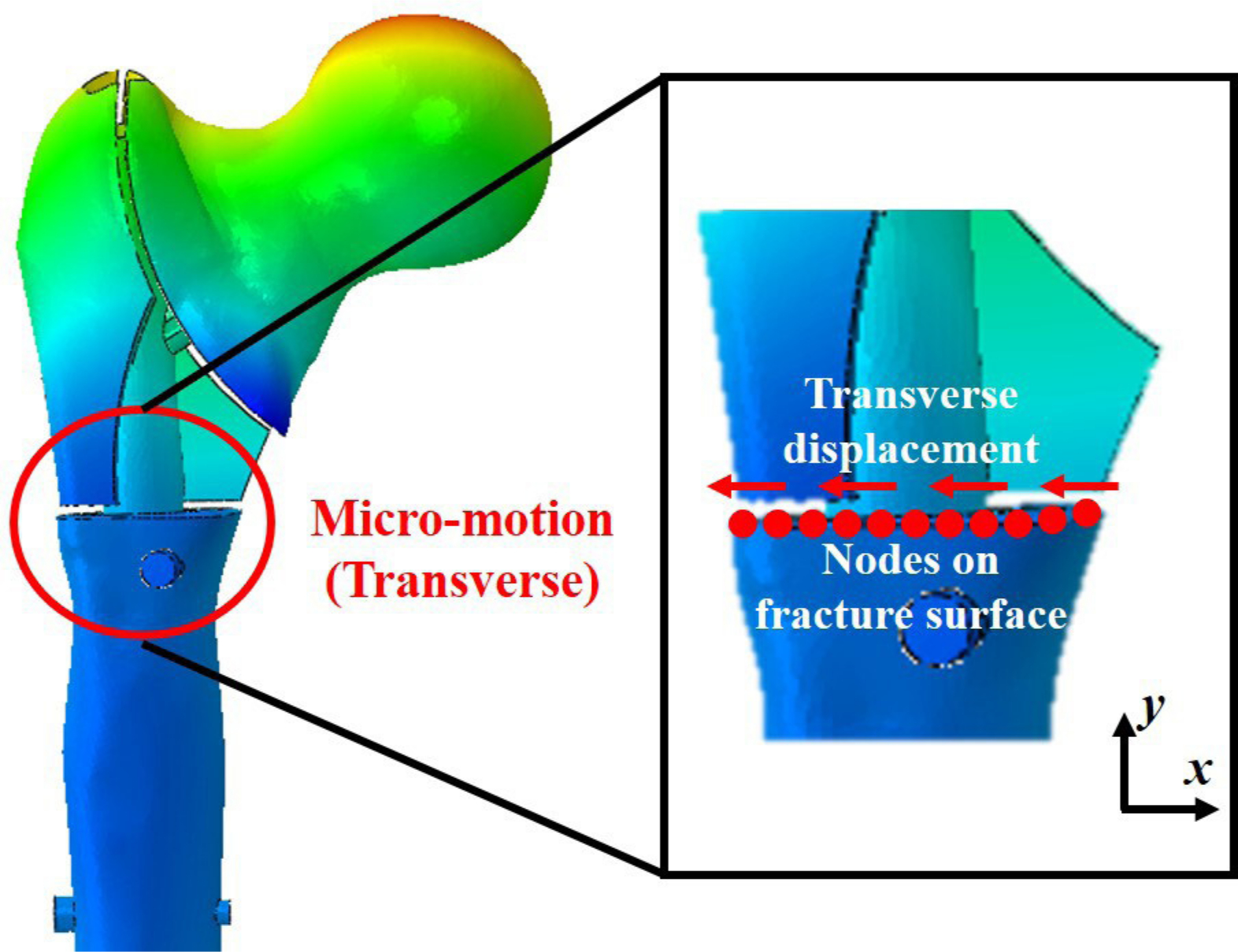
Fig. 3
Micromotion (μm) of the distal fragment related to the proximal fragment was measured through the mean coronal displacement of all nodes on the fracture surface before and after applying axial loading on finite element model.
Stress concentration on CMNs, distal locking screws, and cortical bone was examined. The mean stress over a region of interest (ROI) was measured in each FEM and compared to the yield strength of the nail construct. We set the regions in which the peak von Mises stresses (PVMSs) on the nail, distal locking screw, and cortical bone were observed as the ROIs of each FEM. The yield strength value of the nail-bone construct was referenced from previous studies (TI6A14V, 880 MPa, cortical bone, 114 MPa).22
Results
Micromotions of distal shaft fragment related to proximal fragment
The micromotion of distal shaft fragment related to proximal fragment in each FEM increased as the nail/medullary canal mismatch increased. It also increased when not using a blocking screw. Consequently, the micromotion of distal shaft fragment was the highest in the FEM that had 10 mm nail/medullary canal mismatch without a blocking screw (Figure 4). Micromotions in FEMs without a blocking screw greatly increased as the mismatch increased, whereas micromotions between FEMs with a blocking screw were similar regardless of the mismatch degree. The micromotion reduction rate between FEMs with and without a blocking screw was 81% to 94%, and not consistently related to the degree of nail/medullary canal mismatch.
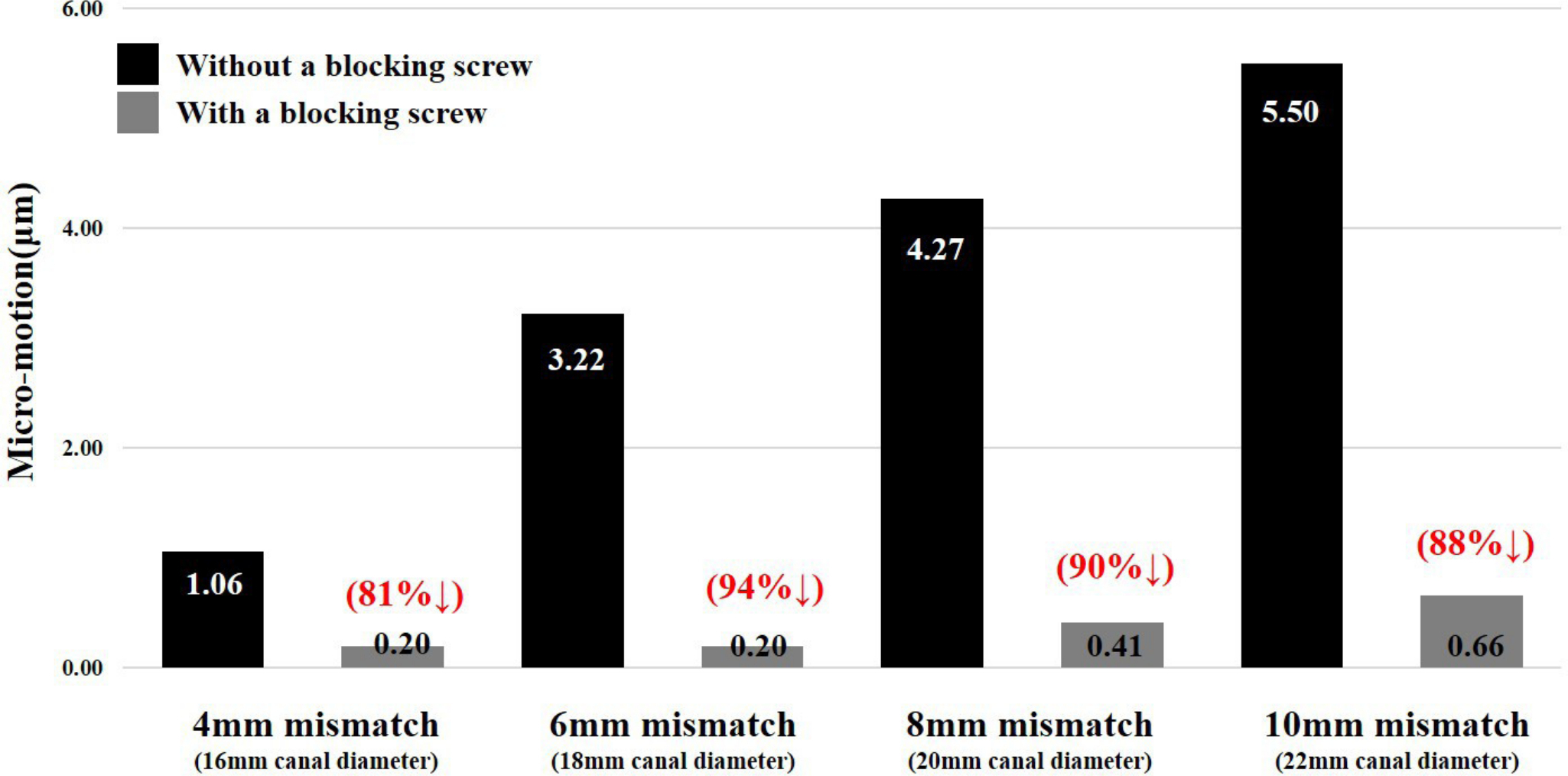
Fig. 4
Micromotion of the distal fragment in each finite element model and reduction rate of the micromotion by using a blocking screw in each model.
Stress distribution on nail body, distal locking screw, and cortical bone
The PVMSs at the nail body in each FEM were observed at the junction of the nail body and lag screw. Therefore, we set the junction of the nail body and the lag screw as the ROI of the nail body in each FEM (Figure 5). Mean stresses over the ROI in FEMs with a blocking screw were lower than those without a blocking screw in all different nail/medullary canal mismatches. The mean stress over a ROI increased as the mismatch increased, regardless of use of a blocking screw. All mean stresses in FEMs with a blocking screw were lower than the yield strength of the nail (TI6A14V, 880 MPa). However, in FEMs without a blocking screw having 8 mm and 10 mm mismatch, mean stresses exceeded the yield strength (1,029 and 1,617 MPa, respectively). The effect of the blocking screw (reduction rate of mean stress) on the nail/medullary canal mismatch increased as the latter increased (19%, 37%, 51%, and 62%, respectively) (Figure 6).
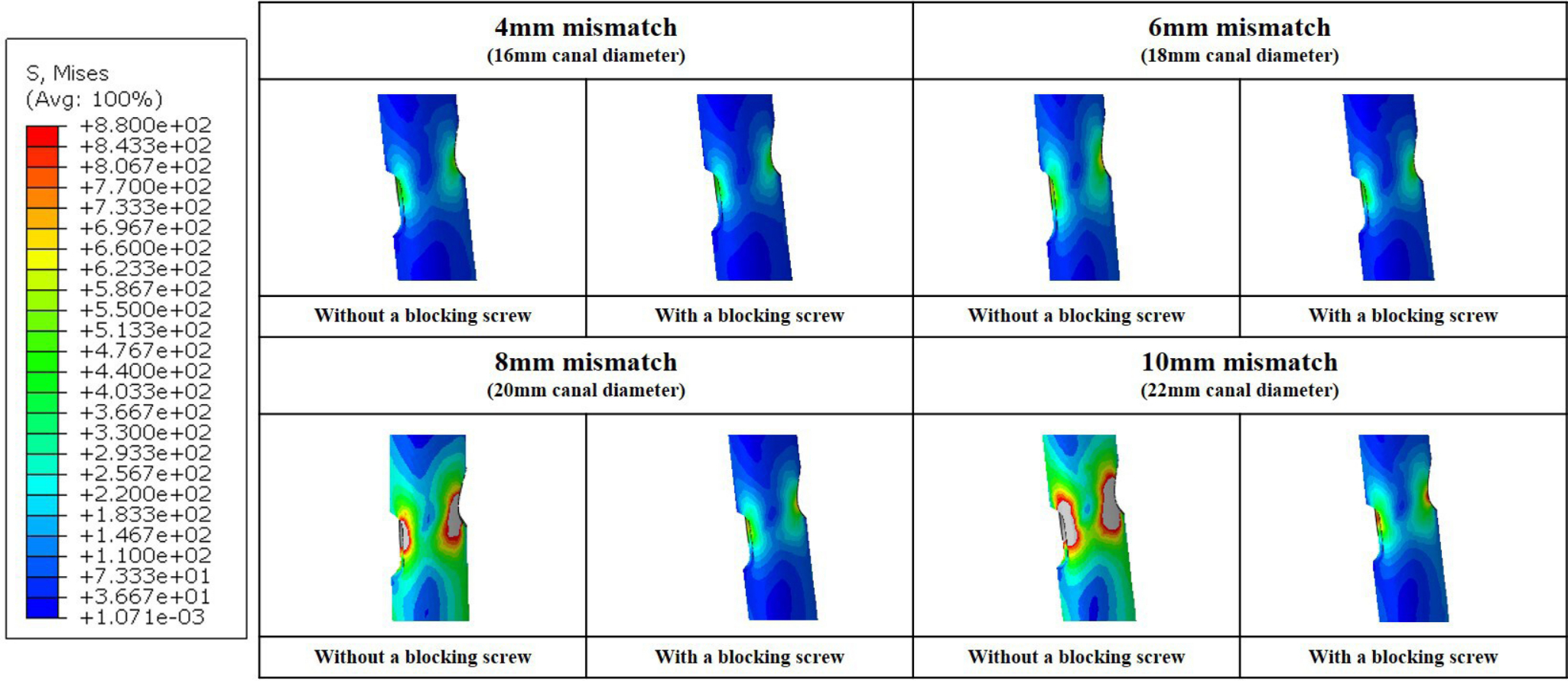
Fig. 5
Stress distribution on the nail body of finite element model. The front view of the junction of the nail body and lag screw.
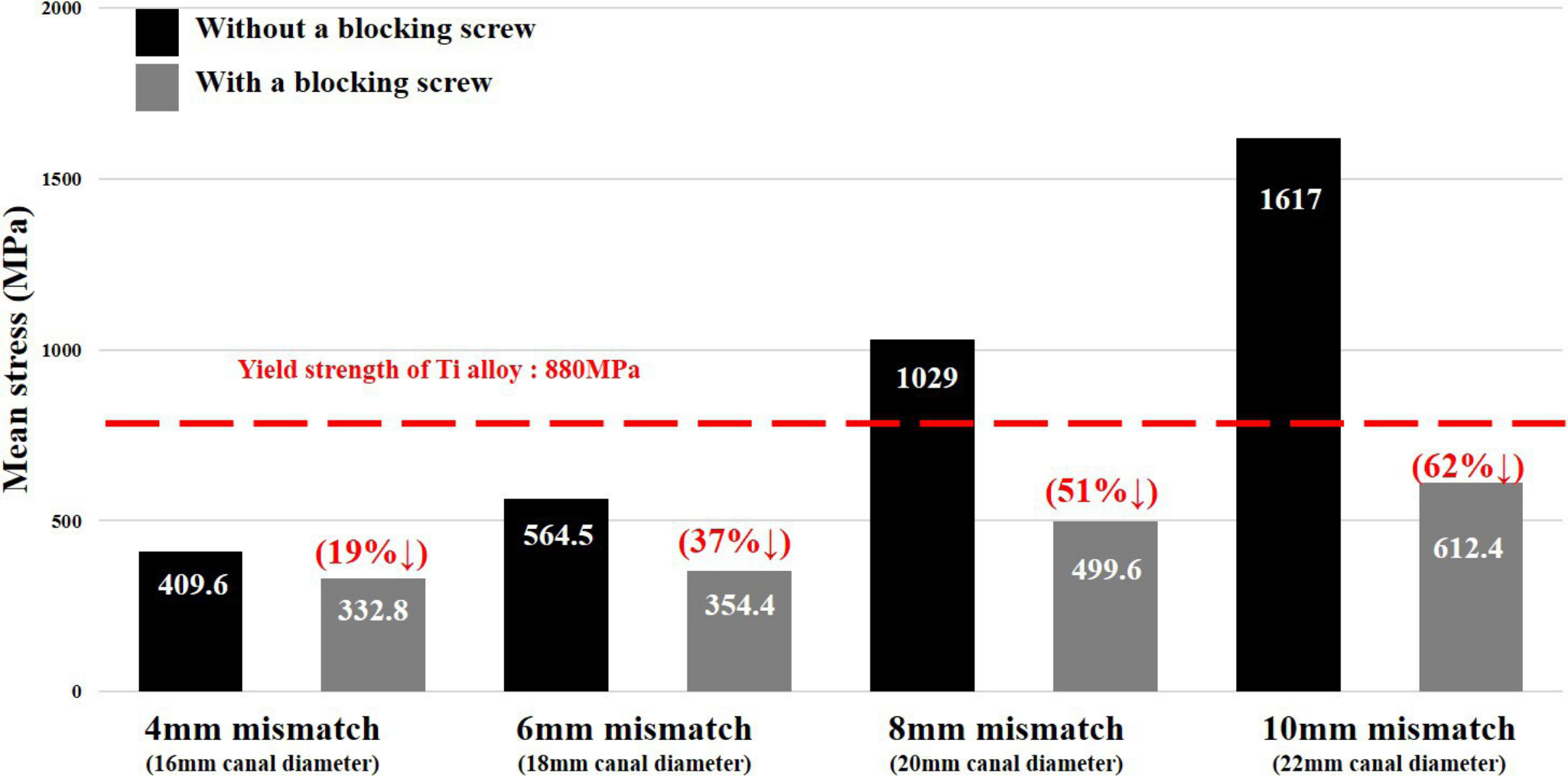
Fig. 6
Mean stress over a region of interest on the nail body in each finite element model and reduction rate of the mean stress by using a blocking screw in each model. MPa, megapascal; Ti, titanium.
The stress concentration at the distal locking screw showed a similar pattern to that observed at the nail body. The PVMS at the distal locking screw in each FEM was observed at the junction of the distal locking screw and medial side of the nail body, which was therefore set as the ROI of the distal locking screw in each FEM (Figure 7). All mean stresses over the ROI in the distal locking screw were lower than those on the ROI of the nail body and yield strength. Figure 8 presents the mean stress over the ROI in each FEM and its reduction rate compared to that over FEMs without a blocking screw.
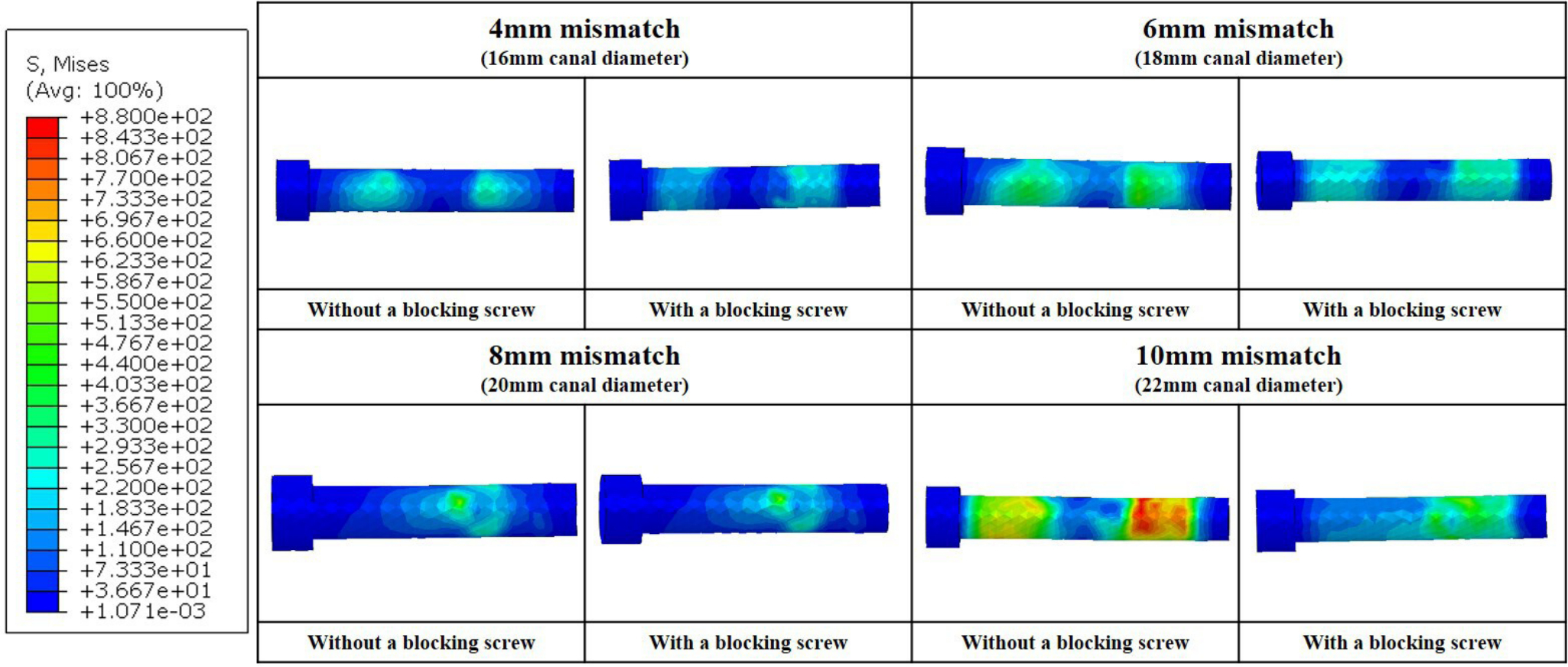
Fig. 7
Stress distribution on the distal locking screw in each finite element model.
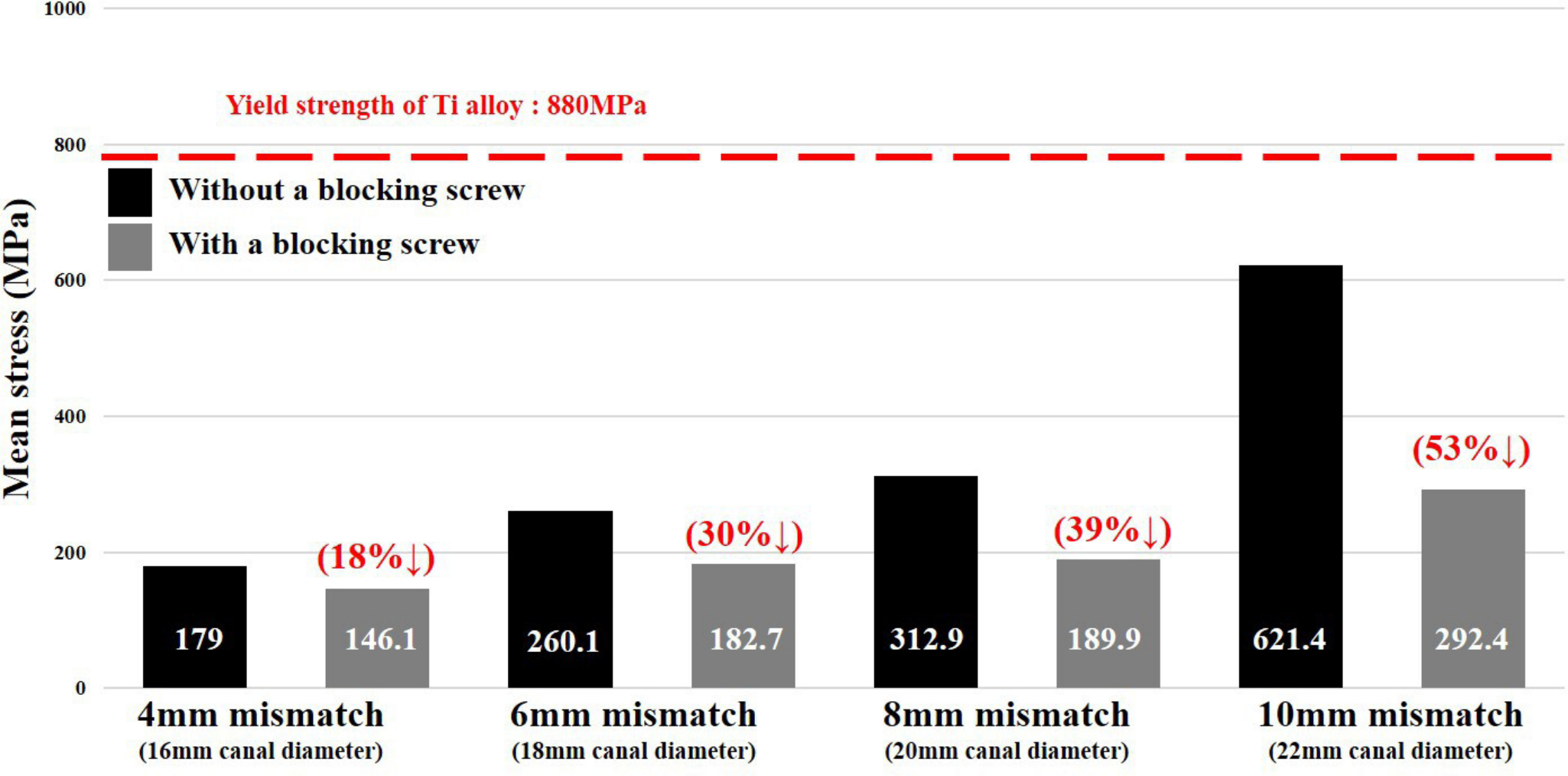
Fig. 8
Mean stress over a region of interest on the distal locking screw in each finite element model and reduction rate of the mean stress by using a blocking screw in each model. MPa, megapascal; Ti, titanium.
The stress concentration on the cortical bone was observed at lateral cortex around the lag screw hole and distal locking screw hole in all FEMs, and it showed a similar pattern to that observed at the nail body and distal locking screw. However, the mean stresses over the ROI in all FEMs were much lower than the yield strength (114 MPa) regardless of the extent of nail/medullary canal mismatch (Supplementary figures a to d).
Discussion
This FEA study revealed that the stress concentration at the nail construct, and micromotions of distal shaft fragment related to proximal fragment, significantly increase as the nail/medullary canal mismatch increases in specific unstable pertrochanteric fracture models fixed with a short CMN. The use of an additional AP blocking screw in these fractures with nail/medullary canal mismatch can greatly reduce stress concentration at the nail construct and micromotions of distal shaft fragment.
Short CMNs have been widely used for the surgical treatment of unstable pertrochanteric fractures due to their biomechanical superiority to extramedullary devices and versatile availability in all fracture types.23 Moreover, short CMNs have yielded favourable results in several studies.24,25
In the ageing population, the medullary canal diameter becomes wider to increase the moment of inertia, and maintain bone stiffness as the cortical bone becomes thinner.26 Consequently, the incidence of pertrochanteric fractures with a wide femoral canal also continues to rise in osteoporotic elderly patients. Nevertheless, the available diameters of CMNs for such fractures are limited and cannot fit all different diameters of the medullary canal, especially in osteoporotic bones with a wide medullary canal. Although CMNs do not need to be press-fit within the medullary canal in most pertrochanteric fractures, mediolateral distal shaft fragment instability may occur due to a nail/medullary canal mismatch after short cephalomedullary nailing for specific unstable pertrochanteric fracture patterns with a wide femoral canal.7,27 Consequently, such a fixation instability may cause excessive distal shaft fragment micromotion, eventually leading to nonunion, fixation failure, or peri-implant fracture. For a large nail/medullary canal mismatch after short cephalomedullary nailing in specific unstable pertrochanteric cases, nail exchange with a long CMN or different short CMNs with two distal locking screws may increase fixation stability. However, this nail exchange takes more time, and may cause greater bleeding and loss of primary reduction status. Moreover, we cannot guarantee that distal shaft fragment mediolateral instability is completely resolved because the largest nail/medullary canal mismatch develops at the metaphyseal-diaphyseal junction. Even if a thicker nail is used, a nail/medullary canal mismatch at the metaphyseal-diaphyseal junction remains unsolved because the proximal diameter of nails is constant regardless of the nail diameter. Accordingly, we believe that a blocking screw around the metaphyseal-diaphyseal junction effectively enhances the stability of the distal fragment in cases of nail/medullary canal mismatch after cephalomedullary nailing in unstable pertrochanteric fractures.
This study revealed that distal shaft fragment micromotions related to the proximal fragment increased as the nail/medullary canal mismatch increased, regardless of blocking screws. However, micromotions in FEMs with a blocking screw showed only slight increases as mismatch increased compared with other FEMs. Meanwhile, micromotions in FEMs without a blocking screw significantly increased as mismatch increased, and this result was consistent with that of the study by Krettek et al.7 They reported that the nail translates along the coronally placed locking screws when a large nail/medullary canal mismatch occurs. As shown in this study, a blocking screw could effectively reduce distal shaft fragment micromotion, that is, mediolateral instability, by up to 94%. The blocking screw also decreased the stress concentration around CMN and was more effective as the nail/medullary canal mismatch increased. Furthermore, the mean stresses over the ROI at the nail body, which were higher than the yield strength in FEMs without a blocking screw having 8 mm and 10 mm mismatch, became less than the yield strength by a blocking screw. Consequently, we believe that using blocking screws can reduce the risk of fixation failure, especially when large nail/medullary canal mismatch occurs. We have used this screw in cases of specific unstable pertrochanteric fractures with a nail/medullary canal mismatch, which show intraoperative instability of the distal shaft fragment.
Previous studies have reported that the use of blocking screws in distal femur fractures or tibia fractures significantly increases distal fragment biomechanical stability, compared with standard fixation with small diameter intramedullary nails.7,28,29 However, to the best of our knowledge, the effect of blocking screws on a nail/medullary canal mismatch after fixation with a short CMN for unstable pertrochanteric fractures has not yet been fully elucidated. We have obtained favourable clinical outcomes using a blocking screw for the aforementioned conditions, although this has not yet been addressed in the literature (Figure 9). Therefore, we believe that our results provide a practical option to resolve this issue for nail/medullary canal mismatch occurring after short CMN fixation for specific unstable pertrochanteric fractures.

Fig. 9
Anteroposterior radiographs taken a) before and b) one year after surgery, showing complete bony union.
There is no guideline or consensus regarding the proper diameter of the blocking screw. The thicker the screw, the greater the subsequent stability. However, in our clinical experiences, it is difficult to insert a thicker screw (4.5 mm) eccentrically into the narrow space between the nail body and bone, especially in poor-quality bone due to, for example, osteoporosis. Moreover, it can increase the risk of blow-out fracture of the distal fragment. Meanwhile, the thinner-diameter (2.7 mm) blocking screw can be insufficient to enhance the stability of the nail-bone construct in large long bone, and we confirmed this possibility through our experimental data. Accordingly, we have used a 3.5 mm cortical screw as the blocking screw clinically in all cases which need the use of a blocking screw, and reported the results using a 3.5 mm cortical screw as the blocking screw in this FEA study. Finally, we believe that a 3.5 mm cortical screw is appropriate as a blocking screw, considering the risk of blow-out fracture and the screw strength in large long bone.
This study has some limitations. First, the complex physiological force components around the proximal femur during normal ambulation were simplified, though physiological loading is more complex, and greater loading can occur in clinical settings. However, only axial loading used to simulate the forces of a one-legged stance was considered appropriate for this FEA, because protected weightbearing with walking aids postoperatively is advised until bony union is achieved. Second, we conducted this study under the linear static condition only. Therefore, we focused on the risk of fixation failure or refracture during the early postoperative period until bony union was achieved, and were unable to consider fatigue fracture requiring long-term cyclic loading. Third, we were unable to determine the exact interaction between the nail and screw, the nail and bone, and the proximal and distal fragments. Although friction coefficients were applied under the assumption of general contact condition at the contact interfaces in the current study, it was difficult to accept these values for perfect reproducibility, as it was challenging to precisely determine these interactions at each interface. Finally, it is difficult to clinically validate our results as this is an experimental study using FEA, and the clinical evidence is still insufficient. However, we believe that this study indicates that the additional AP blocking screw is a viable option to enhance the fixation stability for specific unstable pertrochanteric fractures.
Despite these limitations, a major strength of this study is that it is the first FEA to investigate the effect of an additional AP blocking screw on distal fragment mediolateral instability due to a nail/medullary canal mismatch after short CMN fixation for unstable pertrochanteric fractures. We first investigated stress distribution around the nail construct in unstable pertrochanteric fracture models fixed with a short CMN, and subsequently distal shaft fragment micromotion related to proximal fragment in FEMs with and without a blocking screw. However, further large multicentre clinical studies are needed to confirm our results and verify the availability of blocking screws for specific unstable pertrochanteric fractures with a nail/medullary canal mismatch.
In conclusion, our FEA study revealed that the mean stresses at the nail construct and distal shaft fragment micromotions significantly increase as the nail/medullary canal mismatch increases, and without a blocking screw in unstable pertrochanteric fracture models fixed with a short CMN. The use of an additional AP blocking screw in specific unstable pertrochanteric fractures showing fixation instability due to a nail/medullary canal mismatch after short cephalomedullary nailing can reduce distal fragment micromotion related to proximal fragment and stress concentration at the nail construct. Therefore, an additional AP blocking screw may be a simple and effective alternative to enhance fixation stability in cases of specific unstable pertrochanteric fractures with a large nail/medullary canal mismatch due to osteoporosis.
References
1. Baron JA , Karagas M , Barrett J , et al. Basic epidemiology of fractures of the upper and lower limb among Americans over 65 years of age . Epidemiology . 1996 ; 7 ( 6 ): 612 – 618 . Crossref PubMed Google Scholar
2. Sandmann GH , Biberthaler P . Pertrochanteric femoral fractures in the elderly . Unfallchirurg . 2015 ; 118 ( 5 ): 447 – 460 . Crossref Google Scholar
3. Kokoroghiannis C , Aktselis I , Deligeorgis A , Fragkomichalos E , Papadimas D , Pappadas I . Evolving concepts of stability and intramedullary fixation of intertrochanteric fractures--a review . Injury . 2012 ; 43 ( 6 ): 686 – 693 . Crossref PubMed Google Scholar
4. Han SB , Jung JK , Jang CY , Kwak DK , Kim JW , Yoo JH . Gamma3 nail with U-Blade (RC) lag screw is effective with better surgical outcomes in trochanteric hip fractures . Sci Rep . 2020 ; 10 ( 1 ): 6021 . Crossref PubMed Google Scholar
5. Kim WY , Han CH , Park JI , Kim JY . Failure of intertrochanteric fracture fixation with a dynamic hip screw in relation to pre-operative fracture stability and osteoporosis . Int Orthop . 2001 ; 25 ( 6 ): 360 – 362 . Crossref PubMed Google Scholar
6. Tong X , Burton IS , Isaksson H , Jurvelin JS , Kröger H . Cortical bone histomorphometry in male femoral neck: the investigation of age-association and regional differences . Calcif Tissue Int . 2015 ; 96 ( 4 ): 295 – 306 . Crossref PubMed Google Scholar
7. Krettek C , Stephan C , Schandelmaier P , Richter M , Pape HC , Miclau T . The use of Poller screws as blocking screws in stabilising tibial fractures treated with small diameter intramedullary nails . J Bone Joint Surg Br . 1999 ; 81-B ( 6 ): 963 – 968 . Crossref PubMed Google Scholar
8. Krettek C , Miclau T , Schandelmaier P , Stephan C , Möhlmann U , Tscherne H . The mechanical effect of blocking screws (“Poller screws”) in stabilizing tibia fractures with short proximal or distal fragments after insertion of small-diameter intramedullary nails . J Orthop Trauma . 1999 ; 13 ( 8 ): 550 – 553 . Crossref Google Scholar
9. Kwon GJ , Oh JK , Lee SJ . Effects of screw configuration on biomechanical stability during extra-articular complex fracture fixation of the distal femur treated with locking compression plate . J Biomed Eng Res . 2010 ; 31 : 199 – 209 . Google Scholar
10. Heiner AD , Brown TD . Structural properties of a new design of composite replicate femurs and tibias . J Biomech . 2001 ; 34 ( 6 ): 773 – 781 . Crossref PubMed Google Scholar
11. Köse Ö , Kılıçaslan ÖF , Arık HO , et al. Prediction of osteoporosis through radiographic assessment of proximal femoral morphology and texture in elderly; is it valid and reliable? Turkish Journal of Osteoporosis . 2015 ; 21 ( 2 ): 46 – 52 . Crossref Google Scholar
12. Meinberg EG , Agel J , Roberts CS , Karam MD , Kellam JF . Fracture and dislocation classification compendium-2018 . J Orthop Trauma . 2018 ; 32 Suppl 1 : S1 – S170 . Crossref PubMed Google Scholar
13. Dorr LD , Faugere M-C , Mackel AM , Gruen TA , Bognar B , Malluche HH . Structural and cellular assessment of bone quality of proximal femur . Bone . 1993 ; 14 ( 3 ): 231 – 242 . Crossref PubMed Google Scholar
14. Lee S , Chung CK , Oh SH , Park SB . Correlation between bone mineral density measured by dual-energy X-Ray absorptiometry and hounsfield units measured by diagnostic CT in lumbar spine . J Korean Neurosurg Soc . 2013 ; 54 ( 5 ): 384 – 389 . Crossref PubMed Google Scholar
15. Rho JY , Hobatho MC , Ashman RB . Relations of mechanical properties to density and CT numbers in human bone . Med Eng Phys . 1995 ; 17 ( 5 ): 347 – 355 . Crossref PubMed Google Scholar
16. Morgan EF , Bayraktar HH , Keaveny TM . Trabecular bone modulus-density relationships depend on anatomic site . J Biomech . 2003 ; 36 ( 7 ): 897 – 904 . Crossref PubMed Google Scholar
17. Stoffel K , Dieter U , Stachowiak G , Gächter A , Kuster MS . Biomechanical testing of the LCP--how can stability in locked internal fixators be controlled? Injury . 2003 ; 34 Suppl 2 : B11 - 9 . Crossref PubMed Google Scholar
18. Jiang W , Chen H , Gong JM , Tu ST . Numerical modelling and nanoindentation experiment to study the brazed residual stresses in an X-type lattice truss sandwich structure . Materials Science and Engineering: A . 2011 ; 528 ( 13–14 ): 4715 – 4722 . Crossref Google Scholar
19. Taylor M . Finite element analysis of the resurfaced femoral head . Proc Inst Mech Eng H . 2006 ; 220 ( 2 ): 289 – 297 . Crossref PubMed Google Scholar
20. Law GW , Wong YR , Yew A-S , Choh ACT , Koh JSB , Howe TS . Medial migration in cephalomedullary nail fixation of pertrochanteric hip fractures: a biomechanical analysis using a novel bidirectional cyclic loading model . Bone Joint Res . 2019 ; 8 ( 7 ): 313 – 322 . Crossref PubMed Google Scholar
21. Goffin JM , Pankaj P , Simpson AH . The importance of lag screw position for the stabilization of trochanteric fractures with a sliding hip screw: a subject-specific finite element study . J Orthop Res . 2013 ; 31 ( 4 ): 596 – 600 . Crossref PubMed Google Scholar
22. Merk BR , Stern SH , Cordes S , Lautenschlager EP . A fatigue life analysis of small fragment screws . J Orthop Trauma . 2001 ; 15 ( 7 ): 494 – 499 . Crossref PubMed Google Scholar
23. Nie S , Li M , Ji H , et al. Biomechanical comparison of medial sustainable nail and proximal femoral nail antirotation in the treatment of an unstable intertrochanteric fracture . Bone Joint Res . 2020 ; 9 ( 12 ): 840 – 847 . Crossref PubMed Google Scholar
24. Kregor PJ , Obremskey WT , Kreder HJ , Swiontkowski MF . Unstable pertrochanteric femoral fractures . J Orthop Trauma . 2014 ; 28 Suppl 8 : S25 - 8 . Crossref PubMed Google Scholar
25. Shin YS , Chae JE , Kang TW , Han SB . Prospective randomized study comparing two cephalomedullary nails for elderly intertrochanteric fractures: Zimmer natural nail versus proximal femoral nail antirotation II . Injury . 2017 ; 48 ( 7 ): 1550 – 1557 . Crossref PubMed Google Scholar
26. Pierce MC , Valdevit A , Anderson L , Inoue N , Hauser DL . Biomechanical evaluation of dual-energy X-ray absorptiometry for predicting fracture loads of the infant femur for injury investigation: an in vitro porcine model . J Orthop Trauma . 2000 ; 14 ( 8 ): 571 – 576 . Crossref PubMed Google Scholar
27. Muthusamy S , Rozbruch SR , Fragomen AT . The use of blocking screws with internal lengthening nail and reverse rule of thumb for blocking screws in limb lengthening and deformity correction surgery . Strategies Trauma Limb Reconstr . 2016 ; 11 ( 3 ): 199 – 205 . Crossref PubMed Google Scholar
28. Schumaier AP , Southam BR , Avilucea FR , et al. Factors predictive of blocking screw placement in retrograde nailing of distal femur fractures . J Orthop Trauma . 2019 ; 33 ( 6 ): e229 – e233 . Crossref PubMed Google Scholar
29. Auston D , Donohue D , Stoops K , et al. Long segment blocking screws increase the stability of retrograde nail fixation in geriatric supracondylar femur fractures: eliminating the “Bell-Clapper Effect.” J Orthop Trauma . 2018 ; 32 ( 11 ): 559 – 564 . Crossref Google Scholar
Author contributions
D-K. Kwak: Conceptualization, Writing – original draft.
S-H. Oh: Data curation.
S-J. Lee: Methodology, Supervision.
S-H. Lee: Data curation, Investigation.
Y-M. Lee: Data curation, Investigation.
J-H. Yoo: Conceptualization, Supervision, Writing – review & editing.
Funding statement
The authors disclose receipt of the following financial or material support for the research, authorship, and/or publication of this article: Hallym University Research Fund 2020 (HURF-2020-42).
ICMJE COI statement
There are no conflicts of interest for the authors of the present report.
Open access funding
The authors confirm that the open access fee for this study was self-funded.
Supplementary material
Figures presenting stress distribution and mean stress over a region of interest on the cortical bone.
© 2022 Author(s) et al. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial No Derivatives (CC BY-NC-ND 4.0) licence, which permits the copying and redistribution of the work only, and provided the original author and source are credited. See https://creativecommons.org/licenses/by-nc-nd/4.0/
